Enlarge image
Use your 'Mouse' or the 'Tab' key to move through the fields, except for the "Check Boxes", then you must use the 'Mouse'.
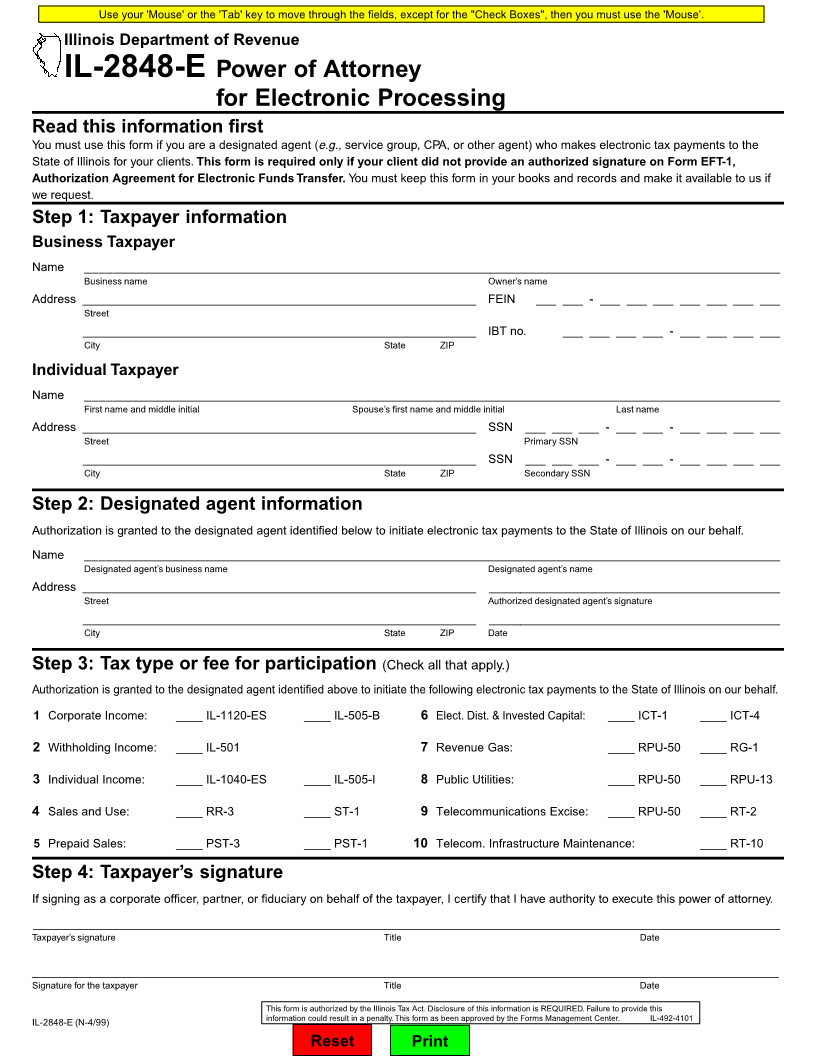
Illinois Department of Revenue
IL-2848-E Power of Attorney
for Electronic Processing
Read this information first
You must use this form if you are a designated agent (e.g., service group, CPA, or other agent) who makes electronic tax payments to the
State of Illinois for your clients. This form is required only if your client did not provide an authorized signature on Form EFT-1,
Authorization Agreement for Electronic Funds Transfer. You must keep this form in your books and records and make it available to us if
we request.
Step 1: Taxpayer information
Business Taxpayer
Name ________________________________________________________________________________________________________
Business name Owner’s name
Address ___________________________________________________________ FEIN ___ ___ - ___ ___ ___ ___ ___ ___ ___
Street
___________________________________________________________ IBT no. ___ ___ ___ ___ - ___ ___ ___ ___
City State ZIP
Individual Taxpayer
Name ________________________________________________________________________________________________________
First name and middle initial Spouse’s first name and middle initial Last name
Address ___________________________________________________________ SSN ___ ___ ___ - ___ ___ - ___ ___ ___ ___
Street Primary SSN
___________________________________________________________ SSN ___ ___ ___ - ___ ___ - ___ ___ ___ ___
City State ZIP Secondary SSN
Step 2: Designated agent information
Authorization is granted to the designated agent identified below to initiate electronic tax payments to the State of Illinois on our behalf.
Name ________________________________________________________________________________________________________
Designated agent’s business name Designated agent’s name
Address ___________________________________________________________ ____________________________________________
Street Authorized designated agent’s signature
___________________________________________________________ ____________________________________________
City State ZIP Date
Step 3: Tax type or fee for participation (Check all that apply.)
Authorization is granted to the designated agent identified above to initiate the following electronic tax payments to the State of Illinois on our behalf.
1 Corporate Income: ____ IL-1120-ES ____ IL-505-B 6 Elect. Dist. & Invested Capital: ____ ICT-1 ____ ICT-4
2 Withholding Income: ____ IL-501 7 Revenue Gas: ____ RPU-50 ____ RG-1
3 Individual Income: ____ IL-1040-ES ____ IL-505-I 8 Public Utilities: ____ RPU-50 ____ RPU-13
4 Sales and Use: ____ RR-3 ____ ST-1 9 Telecommunications Excise: ____ RPU-50 ____ RT-2
5 Prepaid Sales: ____ PST-3 ____ PST-1 10 Telecom. Infrastructure Maintenance: ____ RT-10
Step 4: Taxpayer’s signature
If signing as a corporate officer, partner, or fiduciary on behalf of the taxpayer, I certify that I have authority to execute this power of attorney.
________________________________________________________________________________________________________________
Taxpayer’s signature Title Date
________________________________________________________________________________________________________________
Signature for the taxpayer Title Date
This form is authorized by the Illinois Tax Act. Disclosure of this information is REQUIRED. Failure to provide this
IL-2848-E (N-4/99) information could result in a penalty. This form as been approved by the Forms Management Center. IL-492-4101
Reset Print