Enlarge image
Use your mouse or Tab key to move through the fields. Use your mouse or space bar to enable check boxes.
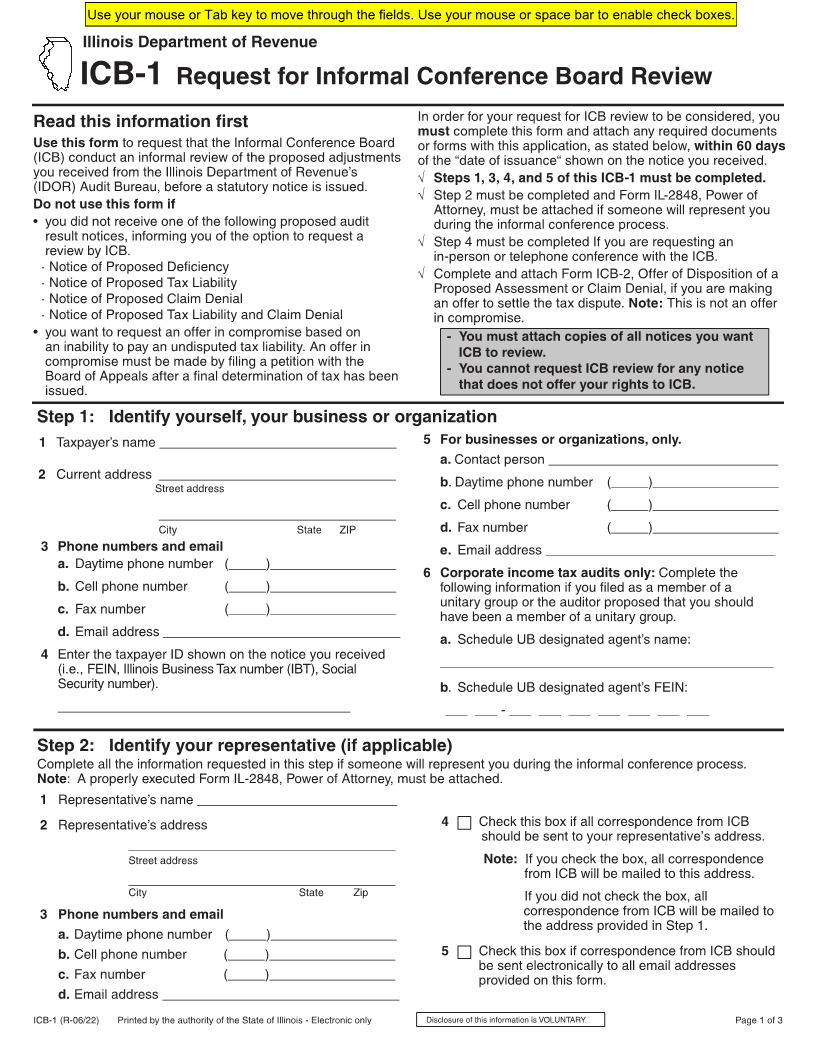
Illinois Department of Revenue
ICB-1 Request for Informal Conference Board Review
In order for your request for ICB review to be considered, you
Read this information first
must complete this form and attach any required documents
Use this form to request that the Informal Conference Board or forms with this application, as stated below, within 60 days
(ICB) conduct of the “datean informalof issuance“ shownreviewonofthethenoticeproposedyou received.adjustments
you received from the Illinois Department of Revenue’s √ Steps 1, 3, 4, and 5 of this ICB-1 must be completed.
(IDOR) Audit Bureau, before a statutory notice is issued.
√ Step 2 must be completed and Form IL-2848, Power of
Do not use this form if Attorney, must be attached if someone will represent you
• you did not receive one of the following proposed audit during the informal conference process.
result notices, informing you of the option to request a √ Step 4 must be completed If you are requesting an
review by ICB. in-person or telephone conference with the ICB.
· Notice of Proposed Deficiency
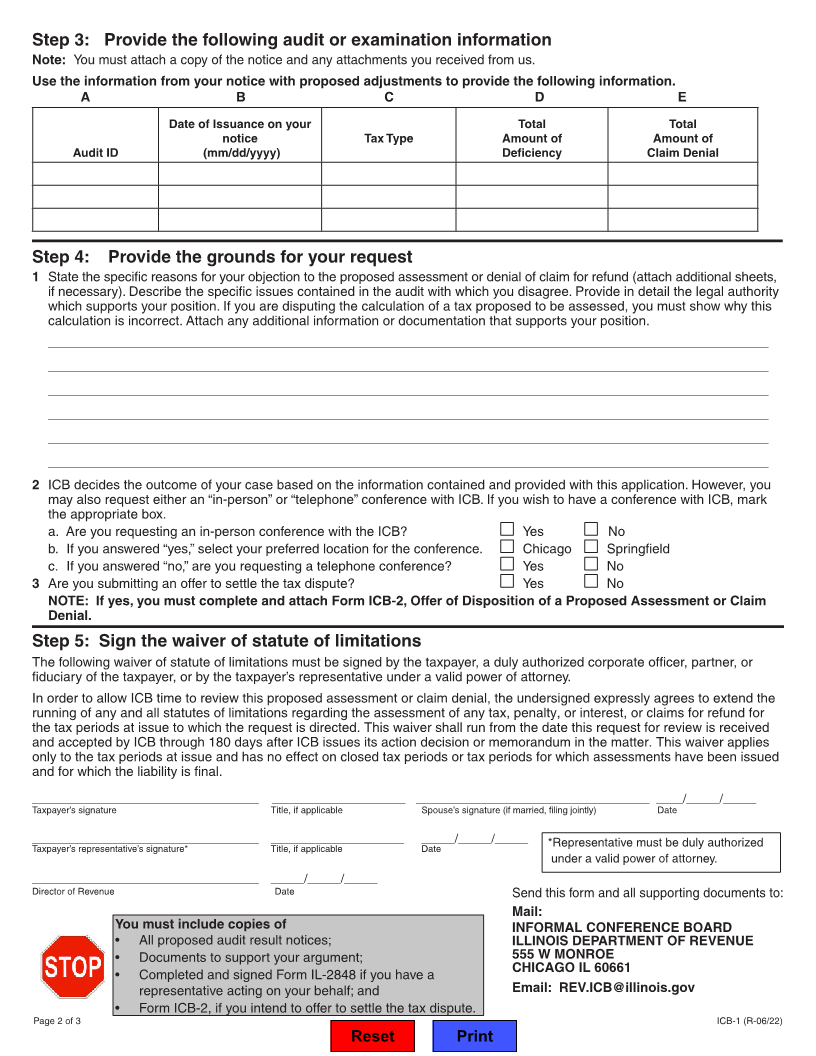
√ Complete and attach Form ICB-2, Offer of Disposition of a
· Notice of Proposed Tax Liability Proposed Assessment or Claim Denial, if you are making
· Notice of Proposed Claim Denial an offer to settle the tax dispute. Note: This is not an offer
· Notice of Proposed Tax Liability and Claim Denial in compromise.
• you want to request an offer in compromise based on - You must attach copies of all notices you want
an inability to pay an undisputed tax liability. An offer in ICB to review.
compromise must be made by filing a petition with the
- You cannot request ICB review for any notice
Board of Appeals after a final determination of tax has been
issued. that does not offer your rights to ICB.
Step 1: Identify yourself, your business or organization
1 Taxpayer’s name ________________________________ 5 For businesses or organizations, only.
a. Contact person _______________________________
2 Current address ________________________________
Street address b. Daytime phone number (_____)_________________
c. Cell phone number (_____)_________________
________________________________
City State ZIP d. Fax number (_____)_________________
3 Phone numbers and email e. Email address _______________________________
a. Daytime phone number (_____)_________________
6 Corporate income tax audits only: Complete the
b. Cell phone number (_____)_________________ following information if you filed as a member of a
unitary group or the auditor proposed that you should
c. Fax number (_____)_________________
have been a member of a unitary group.
d. Email address ________________________________
a. Schedule UB designated agent’s name:
4 Enter the taxpayer ID shown on the notice you received
_____________________________________________
(i.e., FEIN, Illinois Business Tax number (IBT), Social
Security number). b. Schedule UB designated agent’s FEIN:
______________________________________ ___ ___ - ___ ___ ___ ___ ___ ___ ___
Step 2: Identify your representative (if applicable)
Complete all the information requested in this step if someone will represent you during the informal conference process.
Note: A properly executed Form IL-2848, Power of Attorney, must be attached.
1 Representative’s name ___________________________
2 Representative’s address 4 Check this box if all correspondence from ICB
should be sent to your representative’s address.
____________________________________
Street address Note: If you check the box, all correspondence
____________________________________ from ICB will be mailed to this address.
City State Zip If you did not check the box, all
3 Phone numbers and email correspondence from ICB will be mailed to
the address provided in Step 1.
a. Daytime phone number (_____)_________________
b. Cell phone number (_____)_________________ 5 Check this box if correspondence from ICB should
be sent electronically to all email addresses
c. Fax number (_____)_________________ provided on this form.
d. Email address ________________________________
ICB-1 (R-06/22) Printed by the authority of the State of Illinois - Electronic only Disclosure of this information is VOLUNTARY. Page 1 of 3