Enlarge image
Use your 'Mouse' or the 'Tab' key to move through the fields, use your 'Mouse' or 'Space Bar' to enable the "Check Boxes".
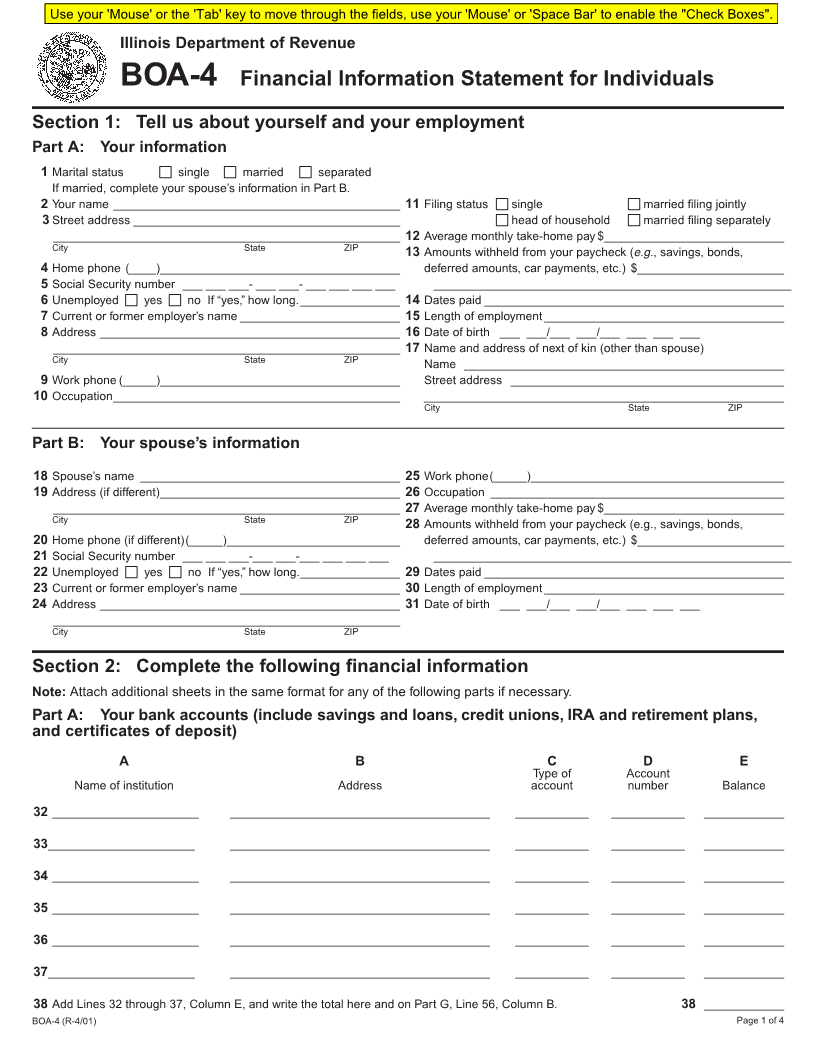
Illinois Department of Revenue
BOA-4 Financial Information Statement for Individuals
Section 1: Tell us about yourself and your employment
Part A: Your information
1 Marital status single married separated
If married, complete your spouse’s information in Part B.
2 Your name ___________________________________________ 11 Filing status single married filing jointly
3Street address ________________________________________ head of household married filing separately
____________________________________________________ 12 Average monthly take-home pay $___________________________
City State ZIP 13 Amounts withheld from your paycheck (e.g., savings, bonds,
4 Home phone (____)____________________________________ deferred amounts, car payments, etc.) $______________________
5 Social Security number ___ ___ ___- ___ ___- ___ ___ ___ ___ ______________________________________________________
6 Unemployed yes no If “yes,” how long._______________ 14 Dates paid _____________________________________________
7 Current or former employer’s name ________________________ 15 Length of employment____________________________________
8 Address _____________________________________________ 16 Date of birth ___ ___/___ ___/___ ___ ___ ___
____________________________________________________ 17 Name and address of next of kin (other than spouse)
City State ZIP Name ________________________________________________
9 Work phone (_____)____________________________________ Street address _________________________________________
10 Occupation___________________________________________ ______________________________________________________
City State ZIP
Part B: Your spouse’s information
18 Spouse’s name _______________________________________ 25 Work phone(_____)______________________________________
19 Address (if different)____________________________________ 26 Occupation ____________________________________________
____________________________________________________ 27 Average monthly take-home pay $___________________________
City State ZIP 28 Amounts withheld from your paycheck (e.g., savings, bonds,
20 Home phone (if different)(_____)__________________________ deferred amounts, car payments, etc.) $______________________
21 Social Security number ___ ___ ___-___ ___-___ ___ ___ ___ ______________________________________________________
22 Unemployed yes no If “yes,” how long._______________ 29 Dates paid _____________________________________________
23 Current or former employer’s name ________________________ 30 Length of employment____________________________________
24 Address _____________________________________________ 31 Date of birth ___ ___/___ ___/___ ___ ___ ___
____________________________________________________
City State ZIP
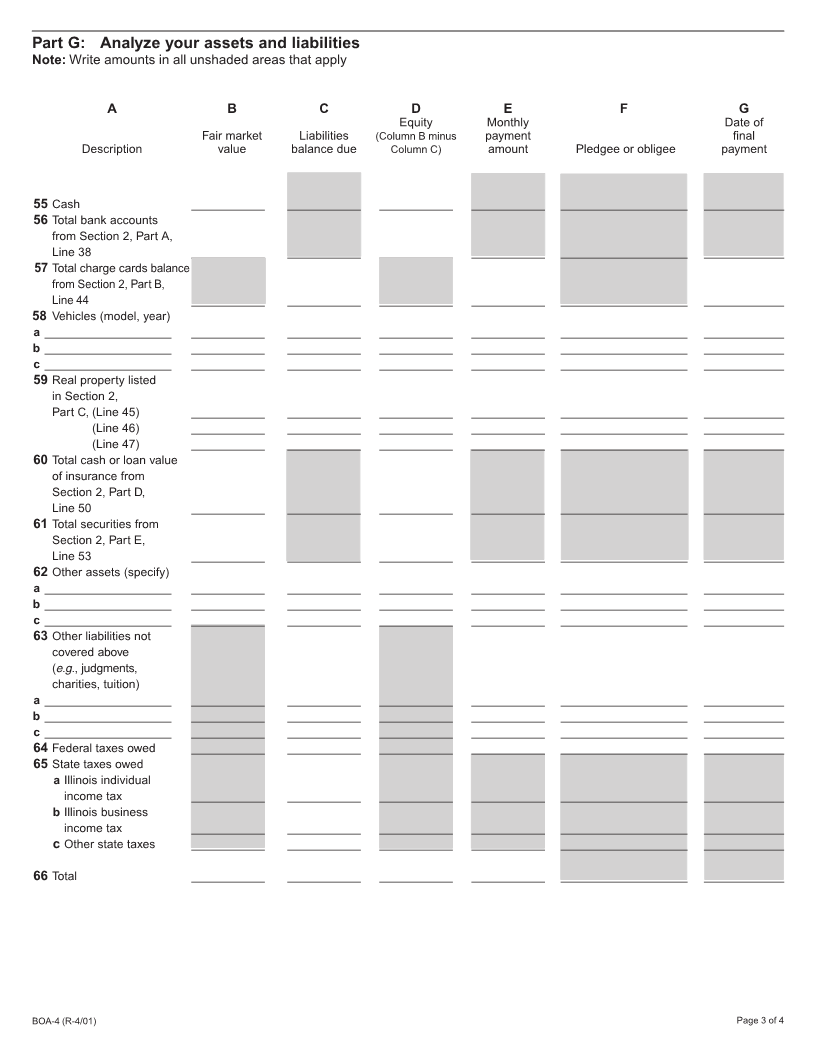
Section 2: Complete the following financial information
Note: Attach additional sheets in the same format for any of the following parts if necessary.
Part A: Your bank accounts (include savings and loans, credit unions, IRA and retirement plans,
and certificates of deposit)
ABCDE
Type of Account
Name of institution Address account number Balance
32 ______________________ _______________________________________ ___________ ___________ ____________
33 ______________________ _______________________________________ ___________ ___________ ____________
34 ______________________ _______________________________________ ___________ ___________ ____________
35 ______________________ _______________________________________ ___________ ___________ ____________
36 ______________________ _______________________________________ ___________ ___________ ____________
37 ______________________ _______________________________________ ___________ ___________ ____________
38 Add Lines 32 through 37, Column E, and write the total here and on Part G, Line 56, Column B. 38 ____________
BOA-4 (R-4/01) Page 1 of 4