Enlarge image
(Do not write in this space) Account #
Subject
Retroactive
Successor
45 South Fruit Street Acquisition
Concord, New Hampshire 03301-4857
Not Subject
Phone (603) 228-4142 Fax (603) 225-4323
www.nhes.nh.gov NAICS
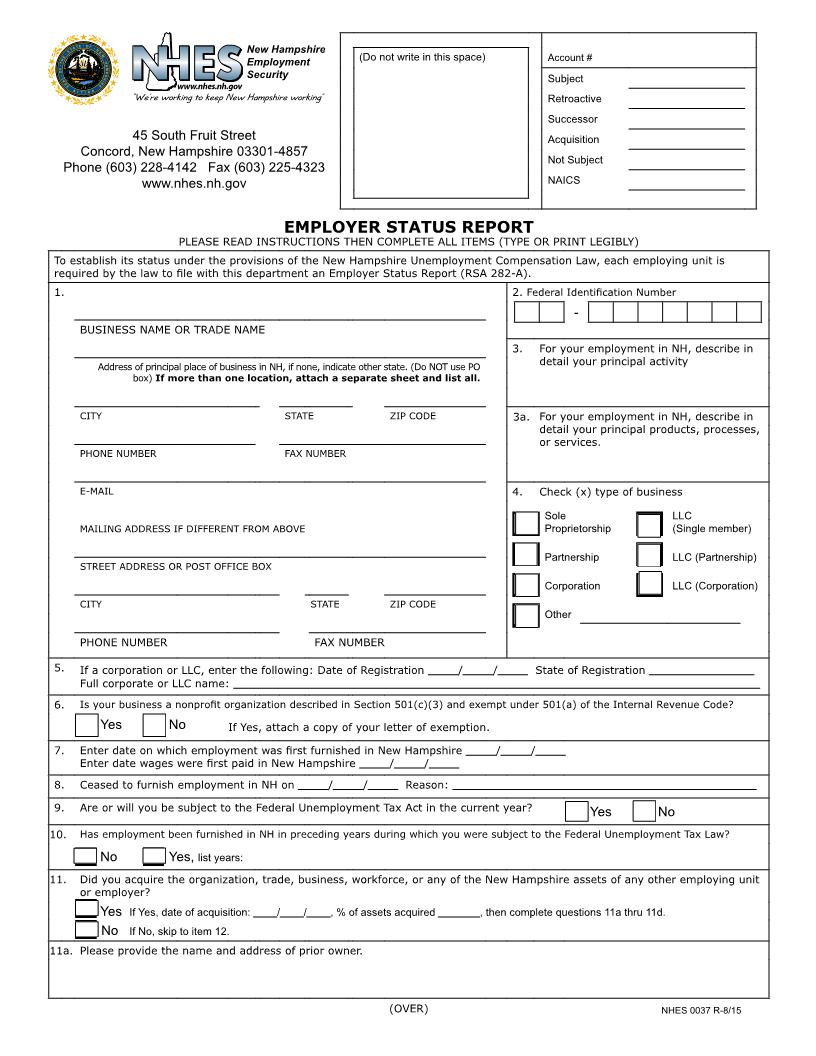
EMPLOYER STATUS REPORT
PLEASE READ INSTRUCTIONS THEN COMPLETE ALL ITEMS (TYPE OR PRINT LEGIBLY)
To establish its status under the provisions of the New Hampshire Unemployment Compensation Law, each employing unit is
required by the law to file with this department an Employer Status Report (RSA 282-A).
1. 2. Federal Identification Number
-
BUSINESS NAME OR TRADE NAME
3. For your employment in NH, describe in
Address of principal place of business in NH, if none, indicate other state. (Do NOT use PO detail your principal activity
box) If more than one location, attach a separate sheet and list all.
CITY STATE ZIP CODE 3a. For your employment in NH, describe in
detail your principal products, processes,
or services.
PHONE NUMBER FAX NUMBER
E-MAIL 4. Check (x) type of business
Sole LLC
MAILING ADDRESS IF DIFFERENT FROM ABOVE Proprietorship (Single member)
Partnership LLC (Partnership)
STREET ADDRESS OR POST OFFICE BOX
Corporation LLC (Corporation)
CITY STATE ZIP CODE
Other
PHONE NUMBER FAX NUMBER
5. If a corporation or LLC, enter the following: Date of Registration / / State of Registration
Full corporate or LLC name:
6. Is your business a nonprofit organization described in Section 501(c)(3) and exempt under 501(a) of the Internal Revenue Code?
Yes No If Yes, attach a copy of your letter of exemption.
7. Enter date on which employment was first furnished in New Hampshire / /
Enter date wages were first paid in New Hampshire / /
8. Ceased to furnish employment in NH on / / Reason:
9. Are or will you be subject to the Federal Unemployment Tax Act in the current year?
Yes No
10. Has employment been furnished in NH in preceding years during which you were subject to the Federal Unemployment Tax Law?
No Yes, list years:
11. Did you acquire the organization, trade, business, workforce, or any of the New Hampshire assets of any other employing unit
or employer?
Yes If Yes, date of acquisition: / / , % of assets acquired , then complete questions 11a thru 11d.
No If No, skip to item 12.
11a. Please provide the name and address of prior owner.
(OVER) NHES 0037 R-8/15