Enlarge image
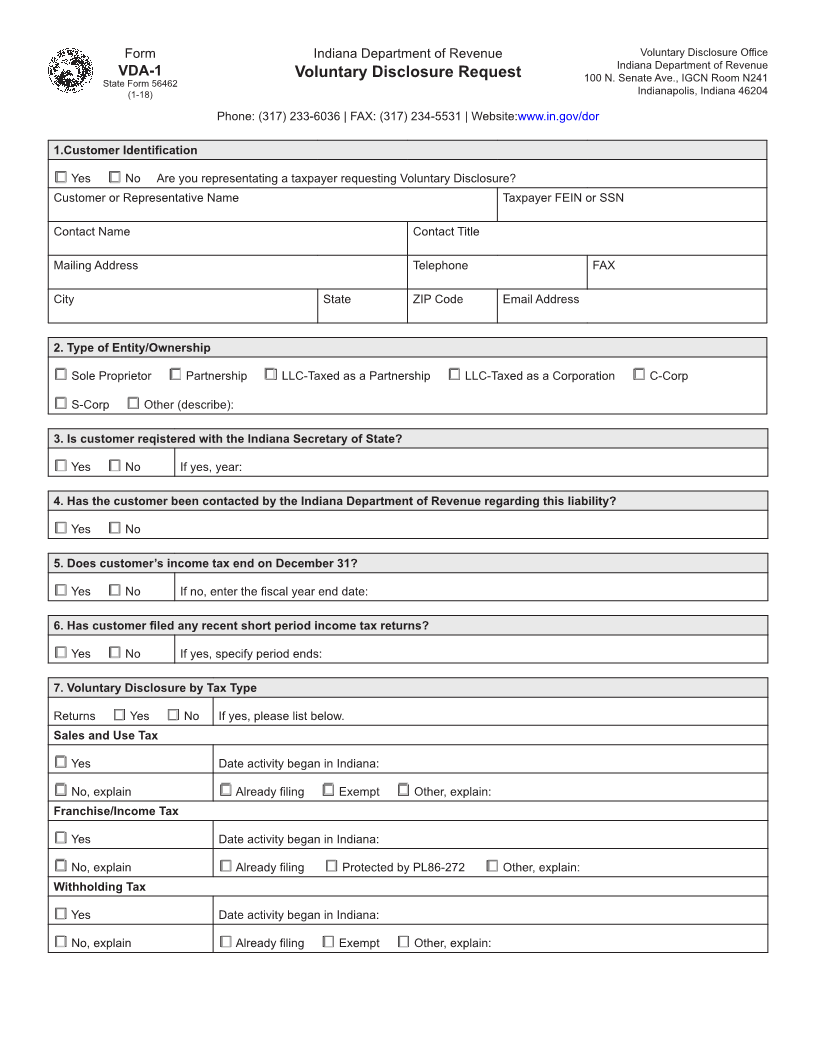
Form Indiana Department of Revenue Voluntary Disclosure Office
Indiana Department of Revenue
VDA-1 Voluntary Disclosure Request 100 N. Senate Ave., IGCN Room N241
State Form 56462
(1-18) Indianapolis, Indiana 46204
Phone: (317) 233-6036 | FAX: (317) 234-5531 | Website:www.in.gov/dor
1.Customer Identification
□ Yes □ No Are you representating a taxpayer requesting Voluntary Disclosure?
Customer or Representative Name Taxpayer FEIN or SSN
Contact Name Contact Title
Mailing Address Telephone FAX
City State ZIP Code Email Address
2. Type of Entity/Ownership
□ Sole Proprietor □ Partnership □ LLC-Taxed as a Partnership □ LLC-Taxed as a Corporation □ C-Corp
□ S-Corp □ Other (describe):
3. Is customer reqistered with the Indiana Secretary of State?
□ Yes □ No If yes, year:
4. Has the customer been contacted by the Indiana Department of Revenue regarding this liability?
□ Yes □ No
5. Does customer’s income tax end on December 31?
□ Yes □ No If no, enter the fiscal year end date:
6. Has customer filed any recent short period income tax returns?
□ Yes □ No If yes, specify period ends:
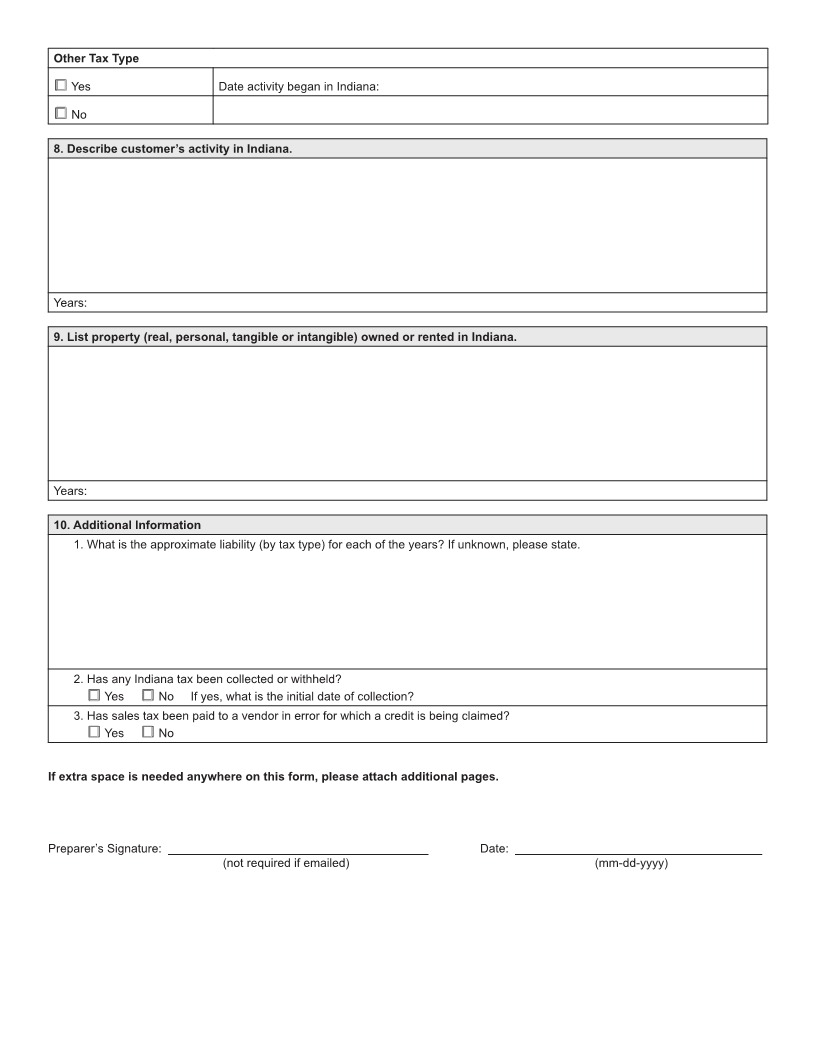
7. Voluntary Disclosure by Tax Type
Returns □ Yes □ No If yes, please list below.
Sales and Use Tax
□ Yes Date activity began in Indiana:
□ No, explain □ Already filing □ Exempt □ Other, explain:
Franchise/Income Tax
□ Yes Date activity began in Indiana:
□ No, explain □ Already filing □ Protected by PL86-272 □ Other, explain:
Withholding Tax
□ Yes Date activity began in Indiana:
□ No, explain □ Already filing □ Exempt □ Other, explain: