Enlarge image
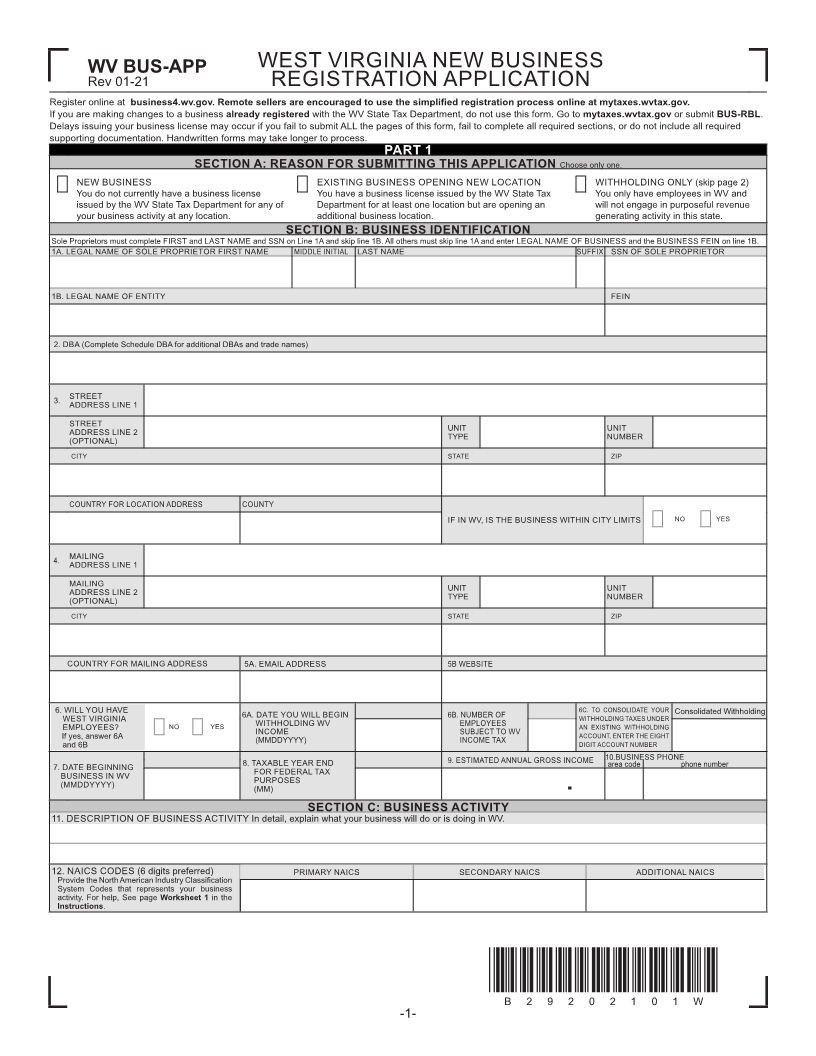
WV BUS-APP WEST VIRGINIA NEW BUSINESS
Rev 01-21 REGISTRATION APPLICATION
Register online at business4.wv.gov. Remote sellers are encouraged to use the simpli edfi registration process online at mytaxes.wvtax.gov.
If you are making changes to a business already registered with the WV State Tax Department, do not use this form. Go to mytaxes.wvtax.gov or submit BUS-RBL.
Delays issuing your business license may occur if you fail to submit ALL the pages of this form, fail to complete all required sections, or do not include all required
supporting documentation. Handwritten forms may take longer to process.
PART 1
SECTION A: REASON FOR SUBMITTING THIS APPLICATION Choose only one.
NEW BUSINESS EXISTING BUSINESS OPENING NEW LOCATION WITHHOLDING ONLY (skip page 2)
You do not currently have a business license You have a business license issued by the WV State Tax You only have employees in WV and
issued by the WV State Tax Department for any of Department for at least one location but are opening an will not engage in purposeful revenue
your business activity at any location. additional business location. generating activity in this state.
SECTION B: BUSINESS IDENTIFICATION
Sole Proprietors must complete FIRST and LAST NAME and SSN on Line 1A and skip line 1B. All others must skip line 1A and enter LEGAL NAME OF BUSINESS and the BUSINESS FEIN on line 1B.
1A. LEGAL NAME OF SOLE PROPRIETOR FIRST NAME MIDDLE INITIAL LAST NAME SUFFIX SSN OF SOLE PROPRIETOR
1B. LEGAL NAME OF ENTITY FEIN
2. DBA (Complete Schedule DBA for additional DBAs and trade names)
3. STREET
ADDRESS LINE 1
STREET UNIT UNIT
ADDRESS LINE 2 TYPE NUMBER
(OPTIONAL)
CITY STATE ZIP
COUNTRY FOR LOCATION ADDRESS COUNTY
IF IN WV, IS THE BUSINESS WITHIN CITY LIMITS NO YES
4. MAILING
ADDRESS LINE 1
MAILING UNIT UNIT
ADDRESS LINE 2 TYPE NUMBER
(OPTIONAL)
CITY STATE ZIP
COUNTRY FOR MAILING ADDRESS 5A. EMAIL ADDRESS 5B WEBSITE
6. WILL YOU HAVE 6A. DATE YOU WILL BEGIN 6B. NUMBER OF 6C. TO CONSOLIDATE YOUR Consolidated Withholding
WEST VIRGINIA WITHHOLDING WV EMPLOYEES WITHHOLDING TAXES UNDER
EMPLOYEES? NO YES INCOME SUBJECT TO WV AN EXISTING WITHHOLDING
If yes, answer 6A (MMDDYYYY) INCOME TAX ACCOUNT, ENTER THE EIGHT
and 6B DIGIT ACCOUNT NUMBER
7. DATE BEGINNING 8. TAXABLE YEAR END 9. ESTIMATED ANNUAL GROSS INCOME 10.BUSINESS PHONE
area code phone number
BUSINESS IN WV FOR FEDERAL TAX
(MMDDYYYY) PURPOSES
(MM) .
SECTION C: BUSINESS ACTIVITY
11. DESCRIPTION OF BUSINESS ACTIVITY In detail, explain what your business will do or is doing in WV.
12. NAICS CODES (6 digits preferred) PRIMARY NAICS SECONDARY NAICS ADDITIONAL NAICS
Provide the North American Industry Classi fication
System Codes that represents your business
activity. For help, See page Worksheet 1 in the
Instructions.
*B29202101W*
B29202101W
-1-