- 4 -
Enlarge image
|
*64112233V*
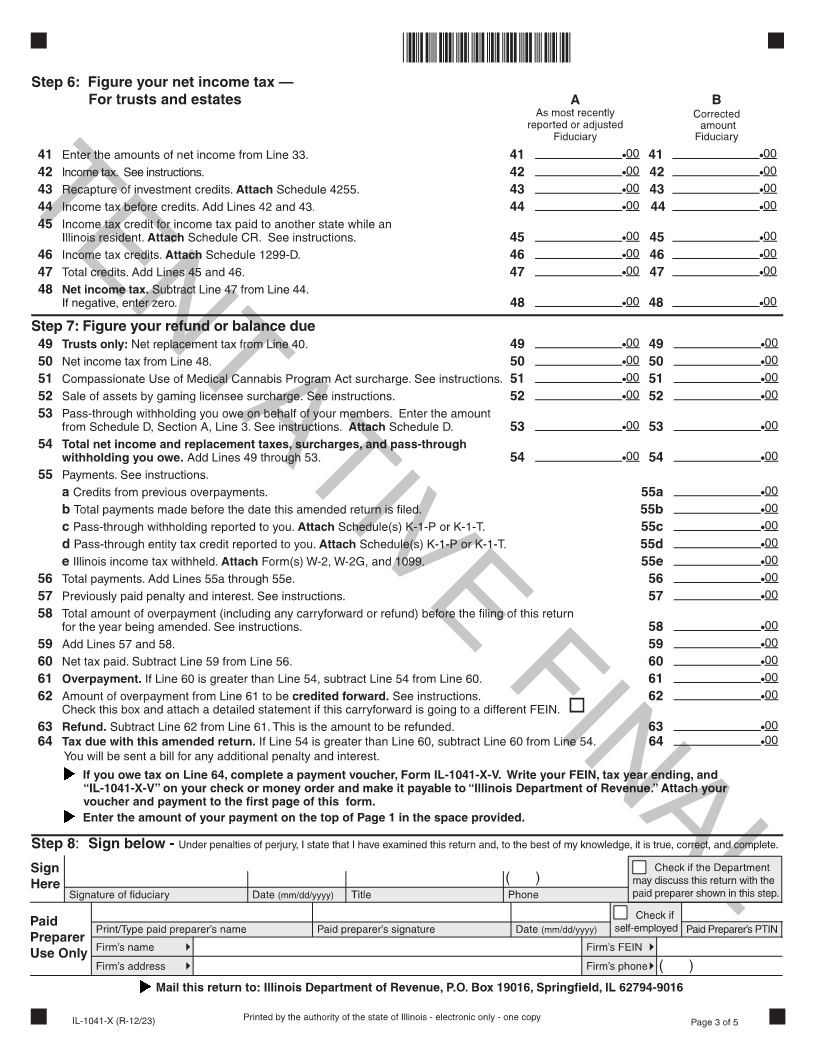
Step 6: Figure your net income tax —
For trusts and estates A B
As most recently Corrected
reported or adjusted amount
Fiduciary Fiduciary
41 Enter the amounts of net income from Line 33. 41 00 41 00
42 Income tax. See instructions. 42 00 42 00
43 Recapture of investment credits. Attach Schedule 4255. 43 00 43 00
44 Income tax before credits. Add Lines 42 and 43. 44 00 44 00
TENTATIVE FINAL
45 Income tax credit for income tax paid to another state while an
Illinois resident. Attach Schedule CR. See instructions. 45 00 45 00
46 Income tax credits. Attach Schedule 1299-D. 46 00 46 00
47 Total credits. Add Lines 45 and 46. 47 00 47 00
48 Net income tax. Subtract Line 47 from Line 44.
If negative, enter zero. 48 00 48 00
Step 7: Figure your refund or balance due
49 Trusts only: Net replacement tax from Line 40. 49 00 49 00
50 Net income tax from Line 48. 50 00 50 00
51 Compassionate Use of Medical Cannabis Program Act surcharge. See instructions. 51 00 51 00
52 Sale of assets by gaming licensee surcharge. See instructions. 52 00 52 00
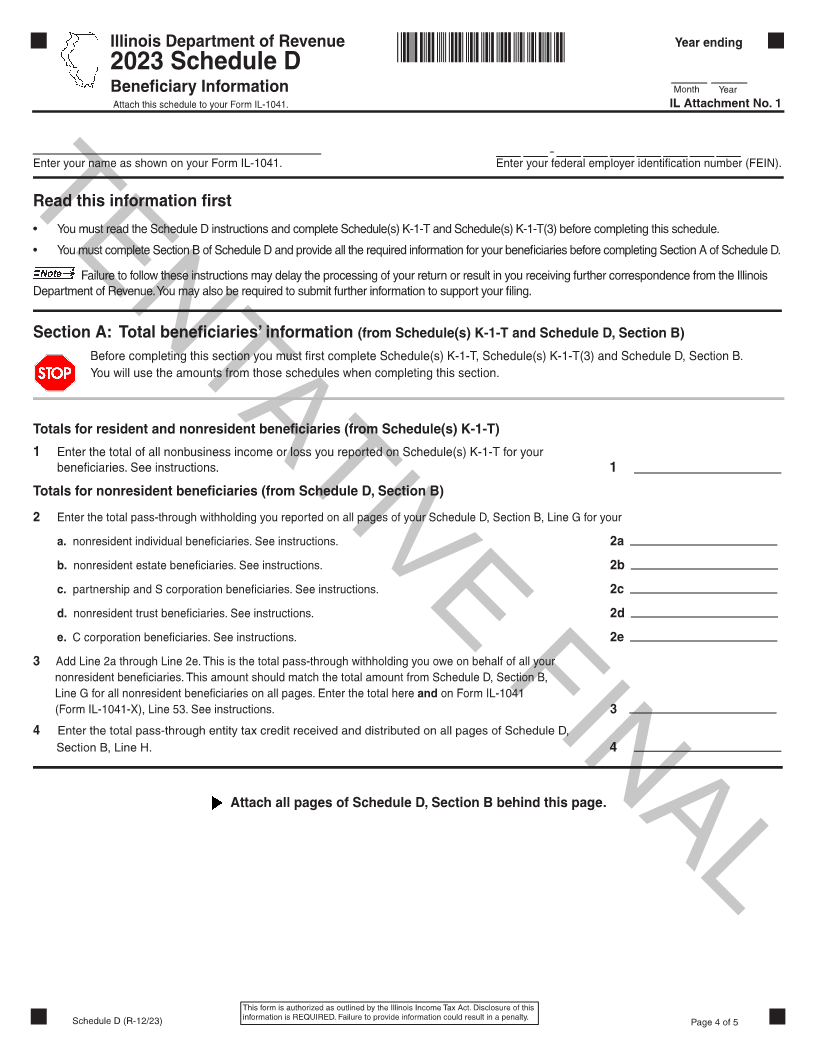
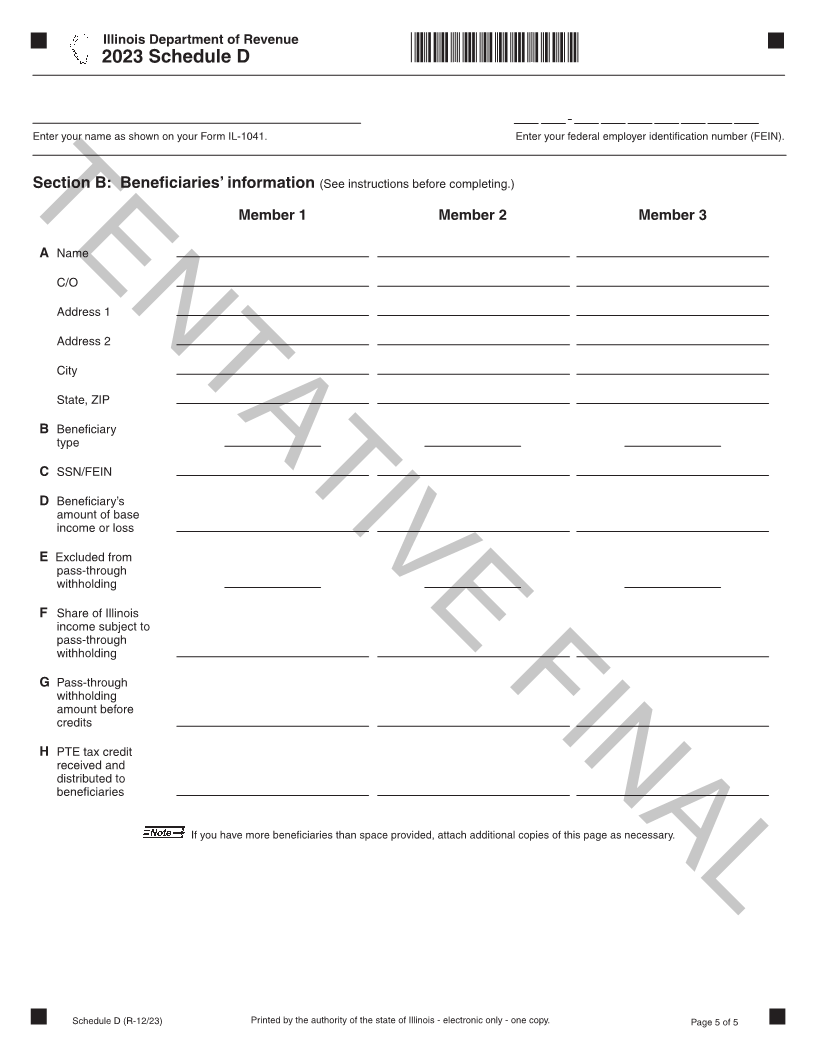
53 Pass-through withholding you owe on behalf of your members. Enter the amount
from Schedule D, Section A, Line 3. See instructions. Attach Schedule D. 53 00 53 00
54 Total net income and replacement taxes, surcharges, and pass-through
withholding you owe. Add Lines 49 through 53. 54 00 54 00
55 Payments. See instructions.
a Credits from previous overpayments. 55a 00
b Total payments made before the date this amended return is filed. 55b 00
c Pass-through withholding reported to you. Attach Schedule(s) K-1-P or K-1-T. 55c 00
d Pass-through entity tax credit reported to you. Attach Schedule(s) K-1-P or K-1-T. 55d 00
e Illinois income tax withheld. Attach Form(s) W-2, W-2G, and 1099. 55e 00
56 Total payments. Add Lines 55a through 55e. 56 00
57 Previously paid penalty and interest. See instructions. 57 00
58 Total amount of overpayment (including any carryforward or refund) before the filing of this return
for the year being amended. See instructions. 58 00
59 Add Lines 57 and 58. 59 00
60 Net tax paid. Subtract Line 59 from Line 56. 60 00
61 Overpayment. If Line 60 is greater than Line 54, subtract Line 54 from Line 60. 61 00
62 Amount of overpayment from Line 61 to be credited forward. See instructions. 62 00
Check this box and attach a detailed statement if this carryforward is going to a different FEIN.
63 Refund. Subtract Line 62 from Line 61. This is the amount to be refunded. 63 00
64 Tax due with this amended return. If Line 54 is greater than Line 60, subtract Line 60 from Line 54. 64 00
You will be sent a bill for any additional penalty and interest.
If you owe tax on Line 64, complete a payment voucher, Form IL-1041-X-V. Write your FEIN, tax year ending, and
“IL-1041-X-V” on your check or money order and make it payable to “Illinois Department of Revenue.” Attach your
voucher and payment to the first page of this form.
Enter the amount of your payment on the top of Page 1 in the space provided.
Step 8: Sign below - Under penalties of perjury, I state that I have examined this return and, to the best of my knowledge, it is true, correct, and complete.
Sign Check if the Department
Here ( ) may discuss this return with the
Signature of fiduciary Date (mm/dd/yyyy) Title Phone paid preparer shown in this step.
Check if
Paid Print/Type paid preparer’s name Paid preparer’s signature Date (mm/dd/yyyy) self-employed Paid Preparer’s PTIN
Preparer
Firm’s name Firm’s FEIN
Use Only
Firm’s address Firm’s phone ( )
Mail this return to: Illinois Department of Revenue, P.O. Box 19016, Springfield, IL 62794-9016
IL-1041-X (R-12/23) Printed by the authority of the state of Illinois - electronic only - one copy Page 3 of 5
|