Enlarge image
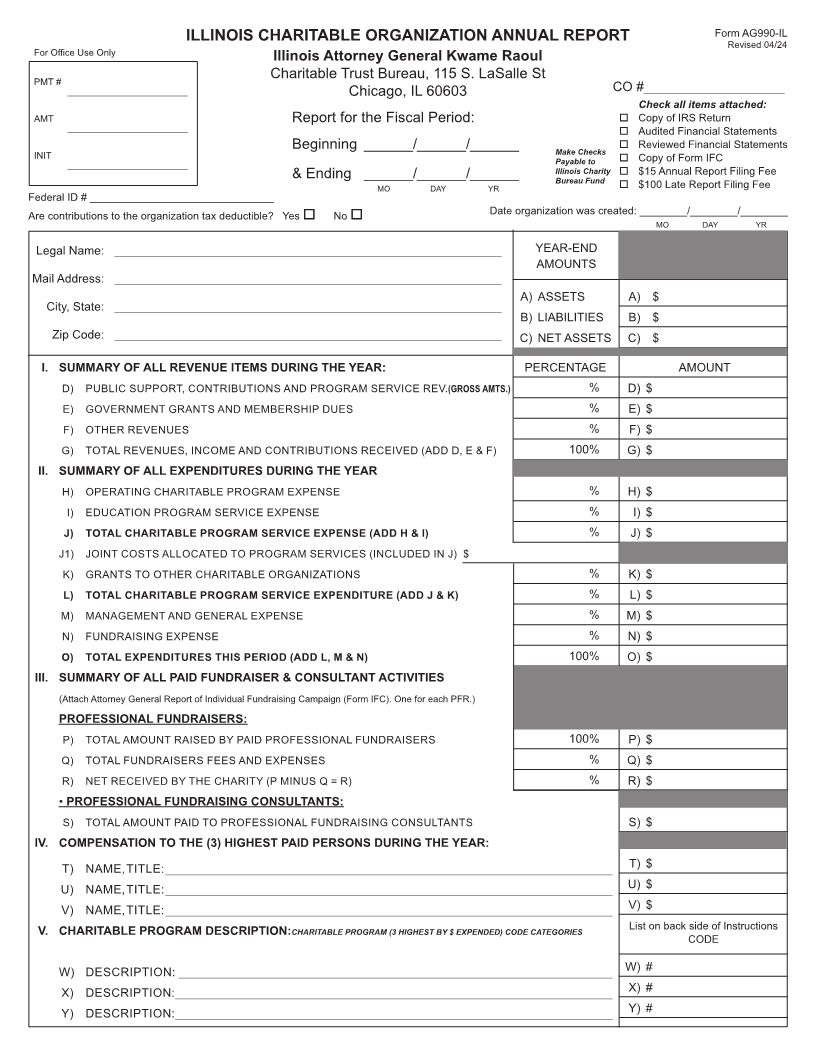
ILLINOIS CHARITABLE ORGANIZATION ANNUAL REPORT Form AG990-IL
Revised 0 /244
For Office Use Only
Illinois Attorney General Kwame Raoul
PMT # Charitable Trust Bureau, 115 S. LaSalle St
___________________________ Chicago, IL 60603 CO #___________________
Check all items attached:
AMT Report for the Fiscal Period: o Copy of IRS Return
___________________________ o Audited Financial Statements
Beginning ______/______/______ Make Checks o Reviewed Financial Statements
INIT Payable to o Copy of Form IFC
___________________________ Illinois Charity o $15 Annual Report Filing Fee
& Ending ______/______/______ Bureau Fund
MO DAY YR o $100 Late Report Filing Fee
Federal ID # _______________________________
Are contributions to the organization tax deductible? Yes o No o Date organization was created: ________/________/________
MO DAY YR
Legal Name: __________________________________________________________ YEAR-END
AMOUNTS
Mail Address: __________________________________________________________
A) ASSETS A) $
City, State: __________________________________________________________
B) LIABILITIES B) $
Zip Code: __________________________________________________________ C) NET ASSETS C) $
I. SUMMARY OF ALL REVENUE ITEMS DURING THE YEAR: PERCENTAGE AMOUNT
D) PUBLIC SUPPORT, CONTRIBUTIONS AND PROGRAM SERVICE REV.(GROSS AMTS.) % D) $
E) GOVERNMENT GRANTS AND MEMBERSHIP DUES % E) $
F) OTHER REVENUES % F) $
G) TOTAL REVENUES, INCOME AND CONTRIBUTIONS RECEIVED (ADD D, E & F) 100% G) $
II. SUMMARY OF ALL EXPENDITURES DURING THE YEAR
H) OPERATING CHARITABLE PROGRAM EXPENSE % H) $
I) EDUCATION PROGRAM SERVICE EXPENSE % I) $
J) TOTAL CHARITABLE PROGRAM SERVICE EXPENSE (ADD H & I) % J) $
J1) JOINT COSTS ALLOCATED TO PROGRAM SERVICES (INCLUDED IN J) $
K) GRANTS TO OTHER CHARITABLE ORGANIZATIONS % K) $
L) TOTAL CHARITABLE PROGRAM SERVICE EXPENDITURE (ADD J & K) % L) $
M) MANAGEMENT AND GENERAL EXPENSE % M) $
N) FUNDRAISING EXPENSE % N) $
O) TOTAL EXPENDITURES THIS PERIOD (ADD L, M & N) 100% O) $
III. SUMMARY OF ALL PAID FUNDRAISER & CONSULTANT ACTIVITIES
(Attach Attorney General Report of Individual Fundraising Campaign (Form IFC). One for each PFR.)
PROFESSIONAL FUNDRAISERS:
P) TOTAL AMOUNT RAISED BY PAID PROFESSIONAL FUNDRAISERS 100% P) $
Q) TOTAL FUNDRAISERS FEES AND EXPENSES % Q) $
R) NET RECEIVED BY THE CHARITY (P MINUS Q = R) % R) $
• PROFESSIONAL FUNDRAISING CONSULTANTS:
S) TOTAL AMOUNT PAID TO PROFESSIONAL FUNDRAISING CONSULTANTS S) $
IV. COMPENSATION TO THE (3) HIGHEST PAID PERSONS DURING THE YEAR:
T) NAME, TITLE: ___________________________________________________________________ T) $
U) NAME, TITLE: ___________________________________________________________________ U) $
V) NAME, TITLE: ___________________________________________________________________ V) $
V. CHARITABLE PROGRAM DESCRIPTION:CHARITABLE PROGRAM (3 HIGHEST BY $ EXPENDED) CODE CATEGORIES List on back side of Instructions
CODE
W) DESCRIPTION: _________________________________________________________________ W) #
X) DESCRIPTION: __________________________________________________________________ X) #
Y) DESCRIPTION: __________________________________________________________________ Y) #
