Enlarge image
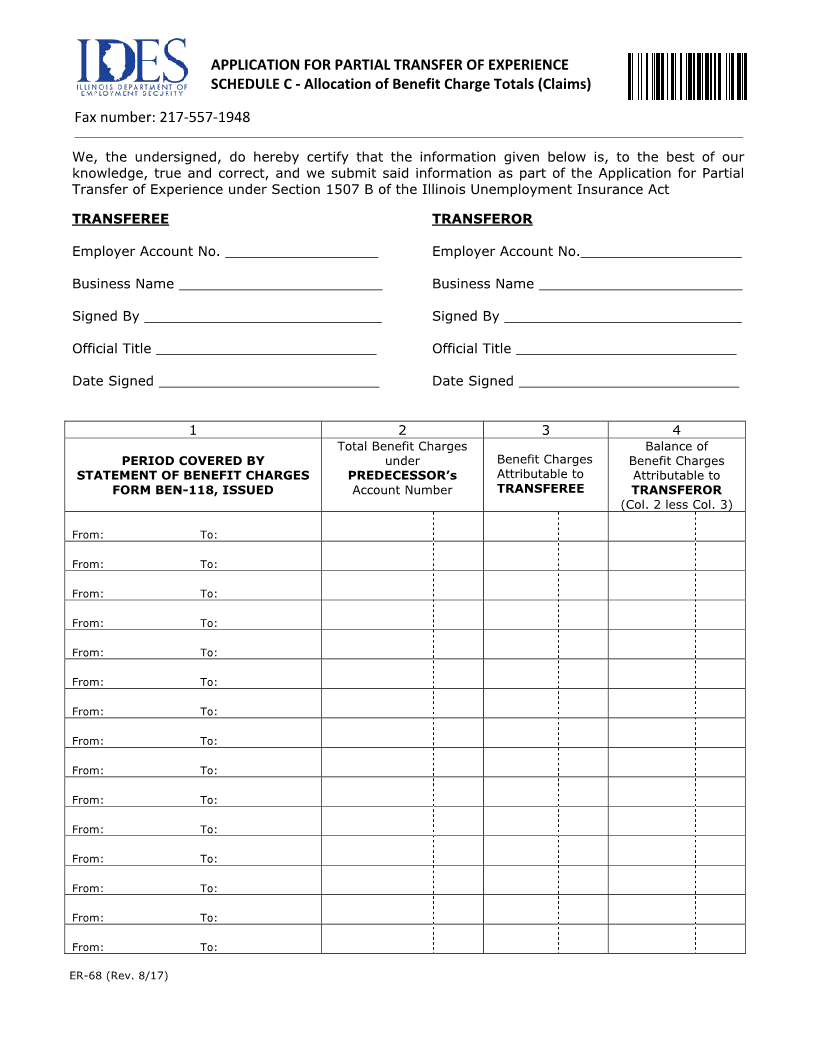
APPLICATION FOR PARTIAL TRANSFER OF EXPERIENCE
SCHEDULE C - Allocation of Benefit Charge Totals (Claims)
Fax number: 217-557-1948
We, the undersigned, do hereby certify that the information given below is, to the best of our
knowledge, true and correct, and we submit said information as part of the Application for Partial
Transfer of Experience under Section 1507 B of the Illinois Unemployment Insurance Act
TRANSFEREE TRANSFEROR
Employer Account No. __________________ Employer Account No.___________________
Business Name ________________________ Business Name ________________________
Signed By ____________________________ Signed By ____________________________
Official Title __________________________ Official Title __________________________
Date Signed __________________________ Date Signed __________________________
1 2 3 4
Total Benefit Charges Balance of
PERIOD COVERED BY under Benefit Charges Benefit Charges
STATEMENT OF BENEFIT CHARGES PREDECESSOR’s Attributable to Attributable to
FORM BEN-118, ISSUED Account Number TRANSFEREE TRANSFEROR
(Col. 2 less Col. 3)
From: To:
From: To:
From: To:
From: To:
From: To:
From: To:
From: To:
From: To:
From: To:
From: To:
From: To:
From: To:
From: To:
From: To:
From: To:
ER-68 (Rev. /8 17)