Enlarge image
Ohio Department of Job and Family Services
Office of Unemployment Insurance Operations
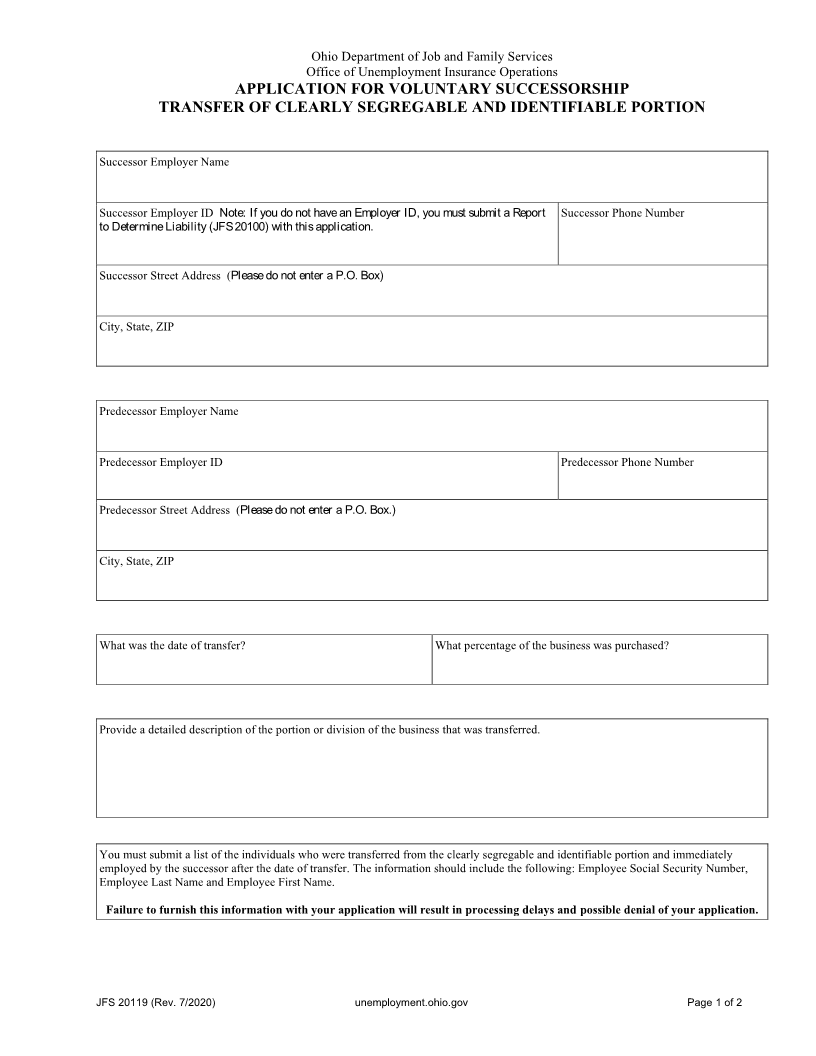
APPLICATION FOR VOLUNTARY SUCCESSORSHIP
TRANSFER OF CLEARLY SEGREGABLE AND IDENTIFIABLE PORTION
Successor Employer Name
Successor Employer ID Note: If you do not have an Employer ID, you must submit a Report Successor Phone Number
to Determine Liability (JFS 20100) with this application.
Successor Street Address (Please do not enter a P.O. Box)
City, State, ZIP
Predecessor Employer Name
Predecessor Employer ID Predecessor Phone Number
Predecessor Street Address (Please do not enter a P.O. Box.)
City, State, ZIP
What was the date of transfer? What percentage of the business was purchased?
Provide a detailed description of the portion or division of the business that was transferred.
You must submit a list of the individuals who were transferred from the clearly segregable and identifiable portion and immediately
employed by the successor after the date of transfer. The information should include the following: Employee Social Security Number,
Employee Last Name and Employee First Name.
Failure to furnish this information with your application will result in processing delays and possible denial of your application.
JFS 20119 (Rev. 7/2020) unemployment.ohio.gov Page 1 of 2