Enlarge image
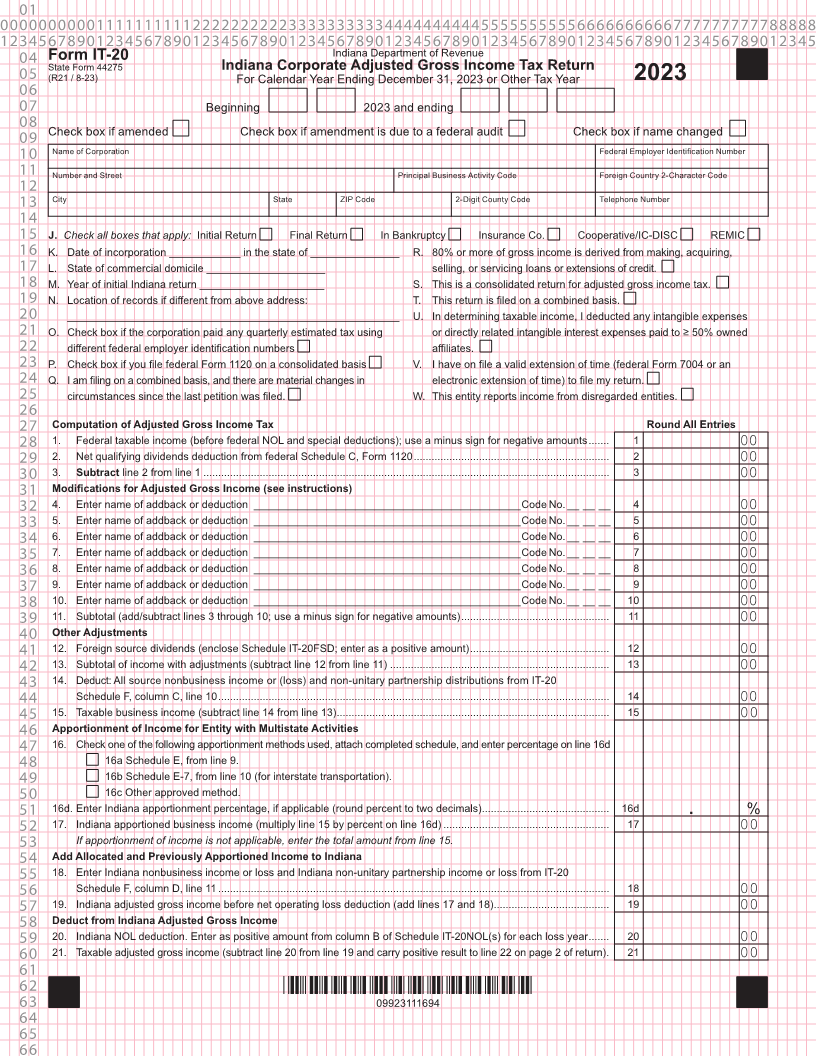
01 0000000000111111111122222222223333333333444444444455555555556666666666777777777788888 1234567890123456789012345678901234567890123456789012345678901234567890123456789012345 04 Form IT-20 Indiana Department of Revenue State Form 44275 Indiana Corporate Adjusted Gross Income Tax Return 05 (R21 / 8-23) For Calendar Year Ending December 31, 2023 or Other Tax Year 2023 06 07 Beginning 2023 and ending 08 Check box if amended Check box if amendment is due to a federal audit Check box if name changed 09 10 Name of Corporation Federal Employer Identification Number 11 Number and Street Principal Business Activity Code Foreign Country 2-Character Code 12 13 City State ZIP Code 2-Digit County Code Telephone Number 14 15 J. Check all boxes that apply: Initial Return Final Return In Bankruptcy Insurance Co. Cooperative/IC-DISC REMIC 16 K. Date of incorporation ____________ in the state of _______________ R. 80% or more of gross income is derived from making, acquiring, 17 L. State of commercial domicile ____________________ selling, or servicing loans or extensions of credit. 18 M. Year of initial Indiana return _____________________ S. This is a consolidated return for adjusted gross income tax. 19 N. Location of records if different from above address: T. This return is filed on a combined basis. 20 ________________________________________________________ U. In determining taxable income, I deducted any intangible expenses 21 O. Check box if the corporation paid any quarterly estimated tax using or directly related intangible interest expenses paid to ≥ 50% owned 22 different federal employer identification numbers affiliates. 23 P. Check box if you file federal Form 1120 on a consolidated basis V. I have on file a valid extension of time (federal Form 7004 or an 24 Q. I am filing on a combined basis, and there are material changes in electronic extension of time) to file my return. 25 circumstances since the last petition was filed. W. This entity reports income from disregarded entities. 26 27 Computation of Adjusted Gross Income Tax Round All Entries 28 1. Federal taxable income (before federal NOL and special deductions); use a minus sign for negative amounts ....... 1 00 29 2. Net qualifying dividends deduction from federal Schedule C, Form 1120 .................................................................. 2 00 30 3. Subtract line 2 from line 1 ......................................................................................................................................... 3 00 31 Modifications for Adjusted Gross Income (see instructions) 32 4. Enter name of addback or deduction _____________________________________________Code No. __ __ __ 4 00 33 5. Enter name of addback or deduction _____________________________________________Code No. __ __ __ 5 00 34 6. Enter name of addback or deduction _____________________________________________Code No. __ __ __ 6 00 35 7. Enter name of addback or deduction _____________________________________________Code No. __ __ __ 7 00 36 8. Enter name of addback or deduction _____________________________________________Code No. __ __ __ 8 00 37 9. Enter name of addback or deduction _____________________________________________Code No. __ __ __ 9 00 38 10. Enter name of addback or deduction _____________________________________________Code No. __ __ __ 10 00 39 11. Subtotal (add/subtract lines 3 through 10; use a minus sign for negative amounts) .................................................. 11 00 40 Other Adjustments 41 12. Foreign source dividends (enclose Schedule IT-20FSD; enter as a positive amount) ............................................... 12 00 42 13. Subtotal of income with adjustments (subtract line 12 from line 11) .......................................................................... 13 00 43 14. Deduct: All source nonbusiness income or (loss) and non-unitary partnership distributions from IT-20 44 Schedule F, column C, line 10 .................................................................................................................................... 14 00 45 15. Taxable business income (subtract line 14 from line 13) ............................................................................................ 15 00 46 Apportionment of Income for Entity with Multistate Activities 47 16. Check one of the following apportionment methods used, attach completed schedule, and enter percentage on line 16d 48 16a Schedule E, from line 9. 49 16b Schedule E-7, from line 10 (for interstate transportation). 50 16c Other approved method. 51 16d. Enter Indiana apportionment percentage, if applicable (round percent to two decimals) ........................................... 16d . % 52 17. Indiana apportioned business income (multiply line 15 by percent on line 16d) ........................................................ 17 00 53 If apportionment of income is not applicable, enter the total amount from line 15. 54 Add Allocated and Previously Apportioned Income to Indiana 55 18. Enter Indiana nonbusiness income or loss and Indiana non-unitary partnership income or loss from IT-20 56 Schedule F, column D, line 11 .................................................................................................................................... 18 00 57 19. Indiana adjusted gross income before net operating loss deduction (add lines 17 and 18) ....................................... 19 00 58 Deduct from Indiana Adjusted Gross Income 59 20. Indiana NOL deduction. Enter as positive amount from column B of Schedule IT-20NOL(s) for each loss year ....... 20 00 60 21. Taxable adjusted gross income (subtract line 20 from line 19 and carry positive result to line 22 on page 2 of return) . 21 00 61 62 *09923111694* 63 09923111694 64 65 66