Enlarge image
Print Form Reset Form
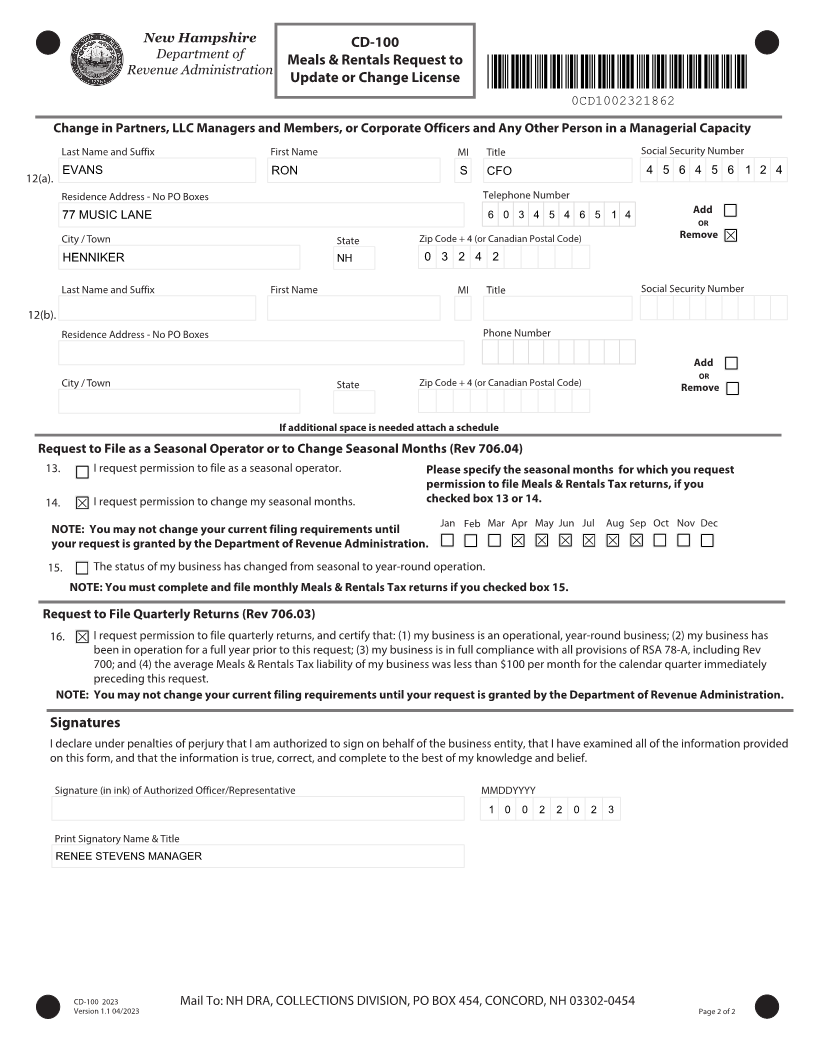
New Hampshire CD-100
Department of Meals & Rentals Request to
Revenue Administration
Update or Change License *0CD1002311862*
0CD1002311862
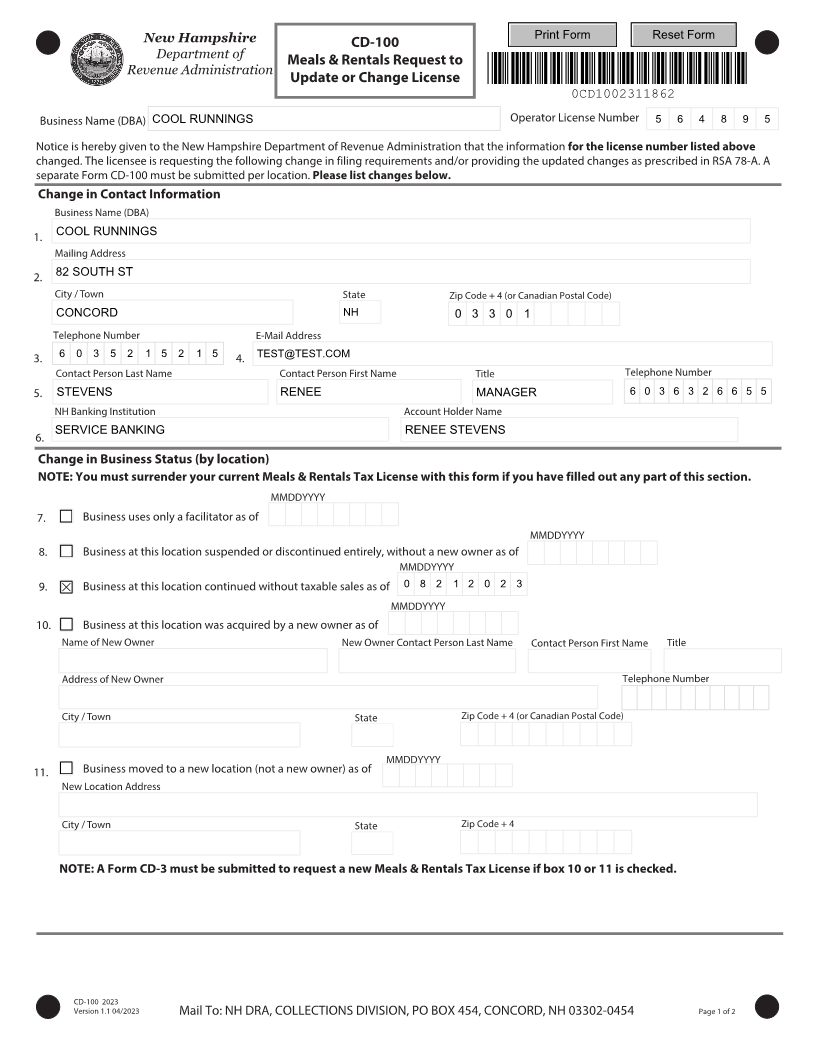
Business Name (DBA) COOL RUNNINGS Operator License Number 5 6 4 8 9 5
Notice is hereby given to the New Hampshire Department of Revenue Administration that the information for the license number listed above
changed. The licensee is requesting the following change in filing requirements and/or providing the updated changes as prescribed in RSA 78-A. A
separate Form CD-100 must be submitted per location. Please list changes below.
Change in Contact Information
Business Name (DBA)
1. COOL RUNNINGS
Mailing Address
2. 82 SOUTH ST
City / Town State Zip Code + 4 (or Canadian Postal Code)
CONCORD NH 0 3 3 0 1
Telephone Number E-Mail Address
3. 6 0 3 5 2 1 5 2 1 5 4. TEST@TEST.COM
Contact Person Last Name Contact Person First Name Title Telephone Number
5. STEVENS RENEE MANAGER 6 0 3 6 3 2 6 6 5 5
NH Banking Institution Account Holder Name
6. SERVICE BANKING RENEE STEVENS
Change in Business Status (by location)
NOTE: You must surrender your current Meals & Rentals Tax License with this form if you have filled out any part of this section.
MMDDYYYY
7. Business uses only a facilitator as of
MMDDYYYY
8. Business at this location suspended or discontinued entirely, without a new owner as of
MMDDYYYY
9. Business at this location continued without taxable sales as of 0 8 2 1 2 0 2 3
MMDDYYYY
10. Business at this location was acquired by a new owner as of
Name of New Owner New Owner Contact Person Last Name Contact Person First Name Title
Address of New Owner Telephone Number
City / Town State Zip Code + 4 (or Canadian Postal Code)
MMDDYYYY
11. Business moved to a new location (not a new owner) as of
New Location Address
City / Town State Zip Code + 4
NOTE: A Form CD-3 must be submitted to request a new Meals & Rentals Tax License if box 10 or 11 is checked.
CD-100 2023
Version 1.1 04/2023 Mail To: NH DRA, COLLECTIONS DIVISION, PO BOX 454, CONCORD, NH 03302-0454 Page 1 of 2