Enlarge image
New Hampshire
Department of DP-175 *0DP1752311862*
Revenue Administration
0DP1752311862
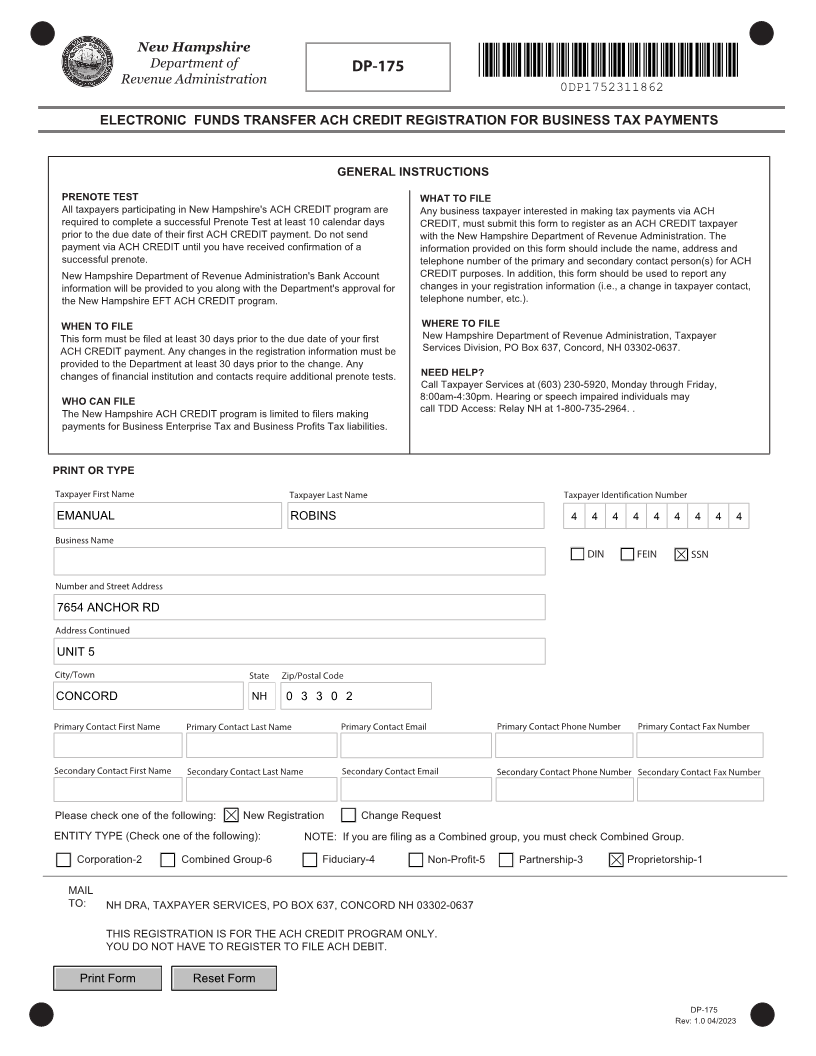
ELECTRONIC FUNDS TRANSFER ACH CREDIT REGISTRATION FOR BUSINESS TAX PAYMENTS
GENERAL INSTRUCTIONS
PRENOTE TEST WHAT TO FILE
All taxpayers participating in New Hampshire's ACH CREDIT program are Any business taxpayer interested in making tax payments via ACH
required to complete a successful Prenote Test at least 10 calendar days CREDIT, must submit this form to register as an ACH CREDIT taxpayer
prior to the due date of their first ACH CREDIT payment. Do not send with the New Hampshire Department of Revenue Administration. The
payment via ACH CREDIT until you have received confirmation of a information provided on this form should include the name, address and
successful prenote. telephone number of the primary and secondary contact person(s) for ACH
New Hampshire Department of Revenue Administration's Bank Account CREDIT purposes. In addition, this form should be used to report any
information will be provided to you along with the Department's approval for changes in your registration information (i.e., a change in taxpayer contact,
the New Hampshire EFT ACH CREDIT program. telephone number, etc.).
WHEN TO FILE WHERE TO FILE
This form must be filed at least 30 days prior to the due date of your first New Hampshire Department of Revenue Administration, Taxpayer
ACH CREDIT payment. Any changes in the registration information must be Services Division, PO Box 637, Concord, NH 03302-0637.
provided to the Department at least 30 days prior to the change. Any
changes of financial institution and contacts require additional prenote tests. NEED HELP?
Call Taxpayer Services at (603) 230-5920, Monday through Friday,
WHO CAN FILE 8:00am-4:30pm. Hearing or speech impaired individuals may
The New Hampshire ACH CREDIT program is limited to filers making call TDD Access: Relay NH at 1-800-735-2964. .
payments for Business Enterprise Tax and Business Profits Tax liabilities.
PRINT OR TYPE
Taxpayer First Name Taxpayer Last Name Taxpayer Identification Number
EMANUAL ROBINS 4 4 4 4 4 4 4 4 4
Business Name
DIN FEIN SSN
Number and Street Address
7654 ANCHOR RD
Address Continued
UNIT 5
City/Town State Zip/Postal Code
CONCORD NH 0 3 3 0 2
Primary Contact First Name Primary Contact Last Name Primary Contact Email Primary Contact Phone Number Primary Contact Fax Number
Secondary Contact First Name Secondary Contact Last Name Secondary Contact Email Secondary Contact Phone NumberSecondary Contact Fax Number
Please check one of the following: New Registration Change Request
ENTITY TYPE (Check one of the following): NOTE: If you are filing as a Combined group, you must check Combined Group.
Corporation-2 Combined Group-6 Fiduciary-4 Non-Profit-5 Partnership-3 Proprietorship-1
MAIL
TO: NH DRA, TAXPAYER SERVICES, PO BOX 637, CONCORD NH 03302-0637
THIS REGISTRATION IS FOR THE ACH CREDIT PROGRAM ONLY.
YOU DO NOT HAVE TO REGISTER TO FILE ACH DEBIT.
Print Form Reset Form
DP-175
Rev: 1. 0 04/2023