Enlarge image
Vermont Department of Taxes
Schedule BI-473 *234731100*
Vermont Composite *234731100*
Page 5
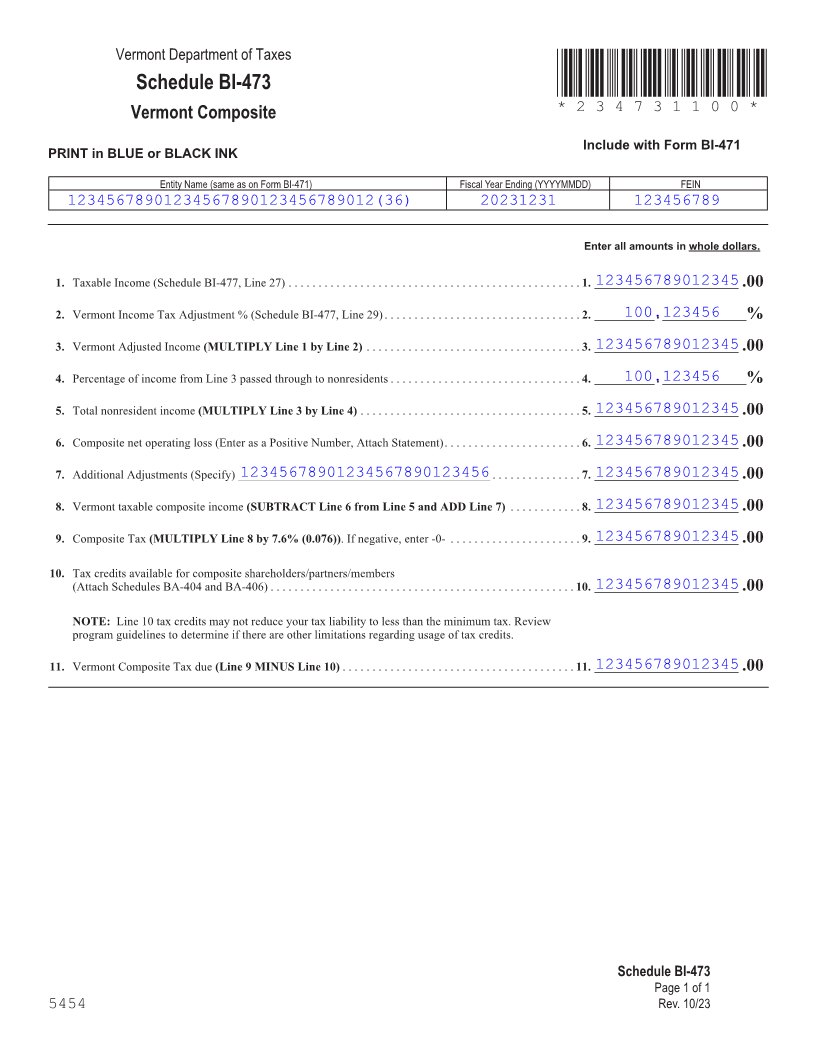
Include with Form BI-471
PRINT in BLUE or BLACK INK
Entity Name (same as on Form BI-471) Fiscal Year Ending (YYYYMMDD) FEIN
12345678901234567890123456789012(36) 20231231 123456789
Enter all amounts in whole dollars.
123456789012345 1. Taxable Income (Schedule BI-477, Line 27) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1. . ________________________.00
100.123456 2. Vermont Income Tax Adjustment % (Schedule BI-477, Line 29) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2. . __________ . ______________%
123456789012345 3. Vermont Adjusted Income(MULTIPLY Line 1 by Line 2) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3. . ________________________.00
100.123456 4. Percentage of income from Line 3 passed through to nonresidents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4. . __________ . ______________%
FORM (Place at FIRST page)
123456789012345 5. Total nonresident income (MULTIPLY Line 3 by Line 4) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5. . ________________________.00 Form pages
123456789012345 6. Composite net operating loss (Enter as a Positive Number, Attach Statement) . . . . . . . . . . . . . . . . . . . . . . 6. . ________________________.00
7. Additional Adjustments (Specify) __________________________________________ 12345678901234567890123456 . . . . . . . . . . . . . . 7. . 123456789012345________________________.00
5 - 5
123456789012345 8. Vermont taxable composite income (SUBTRACT Line 6 from Line 5 and ADD Line 7) . . . . . . . . . . . 8. . ________________________.00
123456789012345 9. Composite Tax (MULTIPLY Line 8 by 7.6% (0.076)) . If negative, enter -0- . . . . . . . . . . . . . . . . . . . . . 9. . ________________________.00
10. Tax credits available for composite shareholders/partners/members
123456789012345(Attach Schedules BA-404 and BA-406) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10. . ________________________.00
NOTE: Line 10 tax credits may not reduce your tax liability to less than the minimum tax . Review
program guidelines to determine if there are other limitations regarding usage of tax credits .
123456789012345 11. Vermont Composite Tax due(Line 9 MINUS Line 10) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11. . ________________________.00
FORM (Place at LAST page)
Form pages
Schedule BI-473 5 - 5
Page 1 of 1
5454 Rev. 10/23