Enlarge image
Clear ALL fields
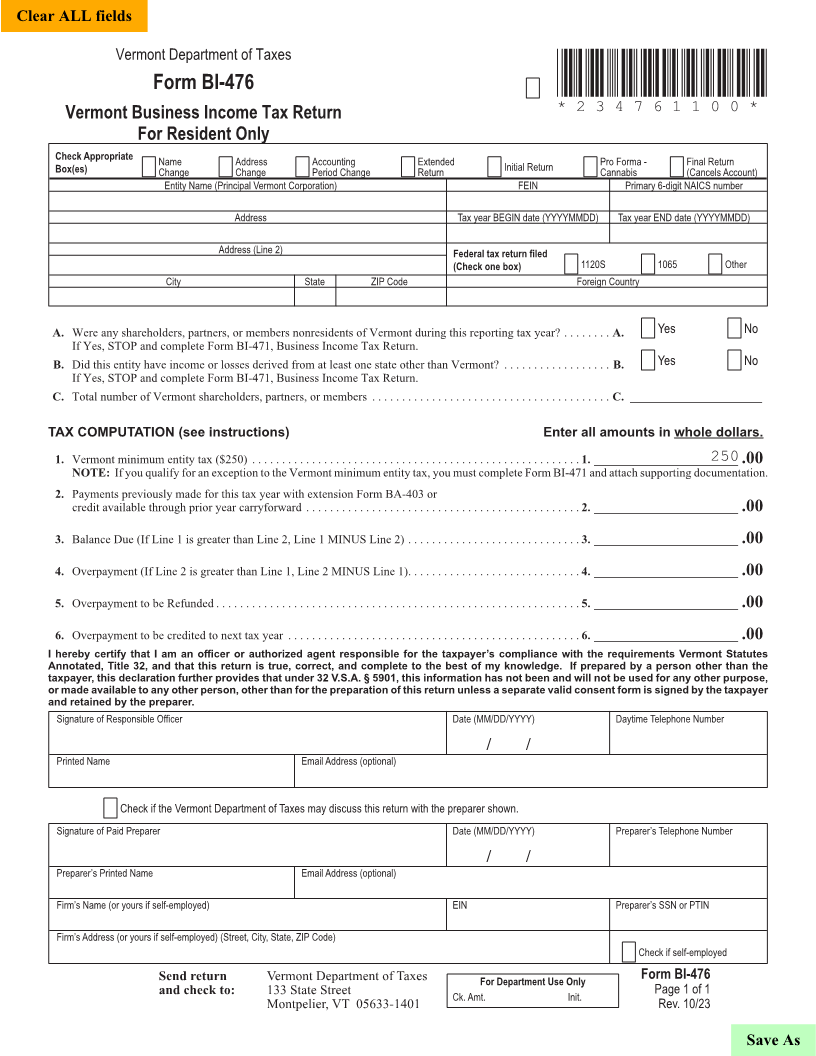
Vermont Department of Taxes
Form BI-476 *234761100*
Vermont Business Income Tax Return *234761100*
Page 5
For Resident Only
Check Appropriate Name Address Accounting Extended Initial Return Pro Forma - Final Return
Box(es) Change Change Period Change Return Cannabis (Cancels Account)
Entity Name (Principal Vermont Corporation) FEIN Primary 6-digit NAICS number
Address Tax year BEGIN date (YYYYMMDD) Tax year END date (YYYYMMDD)
Address (Line 2) Federal tax return filed
(Check one box) 1120S 1065 Other
City State ZIP Code Foreign Country
A. Were any shareholders, partners, or members nonresidents of Vermont during this reporting tax year? . . . . . . . . A. Yes No
If Yes, STOP and complete Form BI-471, Business Income Tax Return .
B. Did this entity have income or losses derived from at least one state other than Vermont? . . . . . . . . . . . . . . . . . . B. Yes No
If Yes, STOP and complete Form BI-471, Business Income Tax Return .
C. Total number of Vermont shareholders, partners, or members . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . C. ______________________ FORM (Place at FIRST page)
Form pages
TAX COMPUTATION (see instructions) Enter all amounts in whole dollars.
1. Vermont minimum entity tax ($250) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1. ________________________250 .00
NOTE: If you qualify for an exception to the Vermont minimum entity tax, you must complete Form BI-471 and attach supporting documentation .
2. Payments previously made for this tax year with extension Form BA-403 or 5 - 5
credit available through prior year carryforward . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2. ________________________ .00
3. Balance Due (If Line 1 is greater than Line 2, Line 1 MINUS Line 2) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3. ________________________ .00
4. Overpayment (If Line 2 is greater than Line 1, Line 2 MINUS Line 1) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4. ________________________ .00
5. Overpayment to be Refunded . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5. ________________________ .00
6. Overpayment to be credited to next tax year . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6. ________________________ .00
I hereby certify that I am an officer or authorized agent responsible for the taxpayer’s compliance with the requirements Vermont Statutes
Annotated, Title 32, and that this return is true, correct, and complete to the best of my knowledge. If prepared by a person other than the
taxpayer, this declaration further provides that under 32 V.S.A. § 5901, this information has not been and will not be used for any other purpose,
or made available to any other person, other than for the preparation of this return unless a separate valid consent form is signed by the taxpayer
and retained by the preparer.
Signature of Responsible Officer Date (MM/DD/YYYY) Daytime Telephone Number
/ /
Printed Name Email Address (optional)
Check if the Vermont Department of Taxes may discuss this return with the preparer shown.
Signature of Paid Preparer Date (MM/DD/YYYY) Preparer’s Telephone Number
/ /
Preparer’s Printed Name Email Address (optional)
FORM (Place at LAST page)
Firm’s Name (or yours if self-employed) EIN Preparer’s SSN or PTIN Form pages
Firm’s Address (or yours if self-employed) (Street, City, State, ZIP Code)
Check if self-employed
Send return Vermont Department of Taxes For Department Use Only Form BI-476
and check to: 133 State Street Ck. Amt. Init. Page 1 of 1 5 - 5
Montpelier, VT 05633-1401 Rev. 10/23
Save As