Enlarge image
01
0000000000111111111122222222223333333333444444444455555555556666666666777777777788888
1234567890123456789012345678901234567890123456789012345678901234567890123456789012345
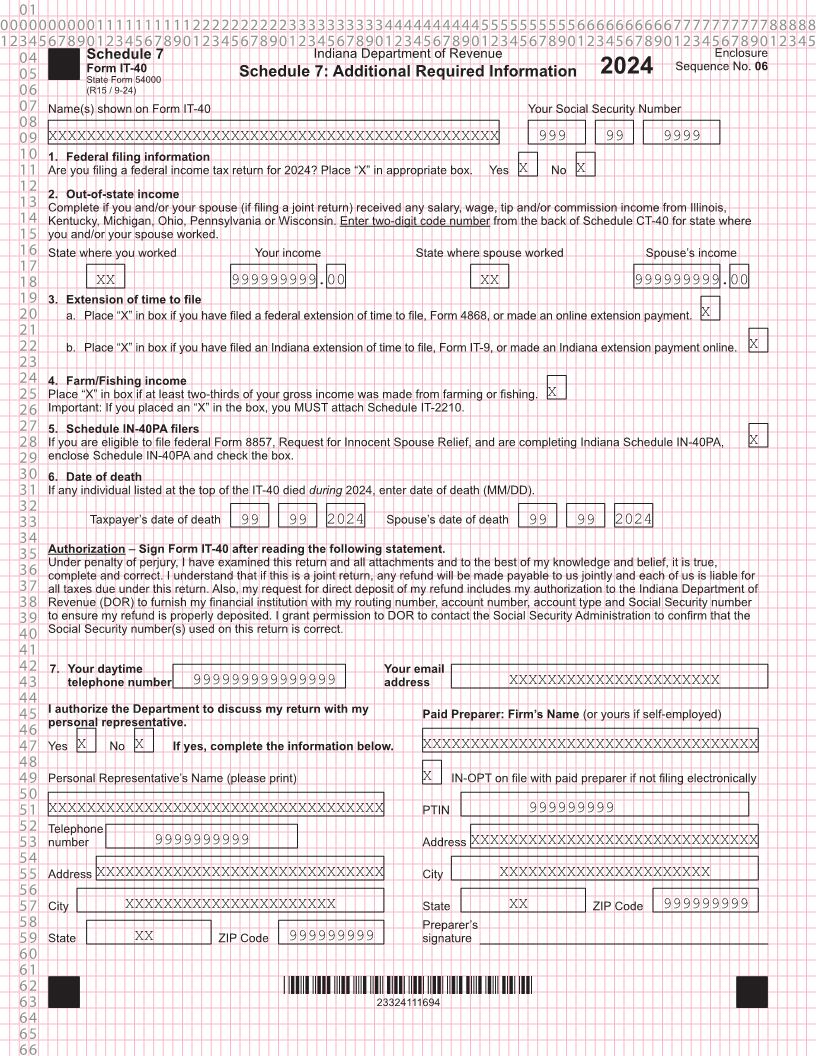
04 Schedule 7 Indiana Department of Revenue Enclosure
Sequence No. 06
05 Form IT-40 Schedule 7: Additional Required Information 2024
State Form 54000
06 (R15 / 9-24)
07 Name(s) shown on Form IT-40 Your Social Security Number
08
09 XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX 999 99 9999
10 1. Federal filing information
11 Are you filing a federal income tax return for 2024? Place “X” in appropriate box. Yes X No X
12
2. Out-of-state income
13 Complete if you and/or your spouse (if filing a joint return) received any salary, wage, tip and/or commission income from Illinois,
14 Kentucky, Michigan, Ohio, Pennsylvania or Wisconsin. Enter two-digit code number from the back of Schedule CT-40 for state where
15 you and/or your spouse worked.
16 State where you worked Your income State where spouse worked Spouse’s income
17
18 XX 999999999.00 XX 999999999 .00
19 3. Extension of time to file
20 a. Place “X” in box if you have filed a federal extension of time to file, Form 4868, or made an online extension payment. X
21
22 b. Place “X” in box if you have filed an Indiana extension of time to file, Form IT-9, or made an Indiana extension payment online. X
23
24 4. Farm/Fishing income
25 Place “X” in box if at least two-thirds of your gross income was made from farming or fishing. X
26 Important: If you placed an “X” in the box, you MUST attach Schedule IT-2210.
27 5. Schedule IN-40PA filers
28 If you are eligible to file federal Form 8857, Request for Innocent Spouse Relief, and are completing Indiana Schedule IN-40PA, X
29 enclose Schedule IN-40PA and check the box.
30 6. Date of death
31 If any individual listed at the top of the IT-40 died during 2024, enter date of death (MM/DD).
32
33 Taxpayer’s date of death 99 99 2024 Spouse’s date of death 99 99 2024
34
35 Authorization – Sign Form IT-40 after reading the following statement.
Under penalty of perjury, I have examined this return and all attachments and to the best of my knowledge and belief, it is true,
36 complete and correct. I understand that if this is a joint return, any refund will be made payable to us jointly and each of us is liable for
37 all taxes due under this return. Also, my request for direct deposit of my refund includes my authorization to the Indiana Department of
38 Revenue (DOR) to furnish my financial institution with my routing number, account number, account type and Social Security number
39 to ensure my refund is properly deposited. I grant permission to DOR to contact the Social Security Administration to confirm that the
40 Social Security number(s) used on this return is correct.
41
42 7. Your daytime Your email
43 telephone number 999999999999999 address XXXXXXXXXXXXXXXXXXXXXX
44
45 I authorize the Department to discuss my return with my Paid Preparer: Firm’s Name (or yours if self-employed)
personal representative.
46
47 Yes X No X If yes, complete the information below. XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
48
49 Personal Representative’s Name (please print) X IN-OPT on file with paid preparer if not filing electronically
50
51 XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX PTIN 999999999
52 Telephone
53 number 9999999999 Address XXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
54
55 Address XXXXXXXXXXXXXXXXXXXXXXXXXXXXXX City XXXXXXXXXXXXXXXXXXXXXX
56
57 City XXXXXXXXXXXXXXXXXXXXXX State XX ZIP Code 999999999
58 Preparer’s
59 State XX ZIP Code 999999999 signature
60
61
62 *23324111694*
63 23324111694
64
65
66