Enlarge image
01
0000000000111111111122222222223333333333444444444455555555556666666666777777777788888
1234567890123456789012345678901234567890123456789012345678901234567890123456789012345
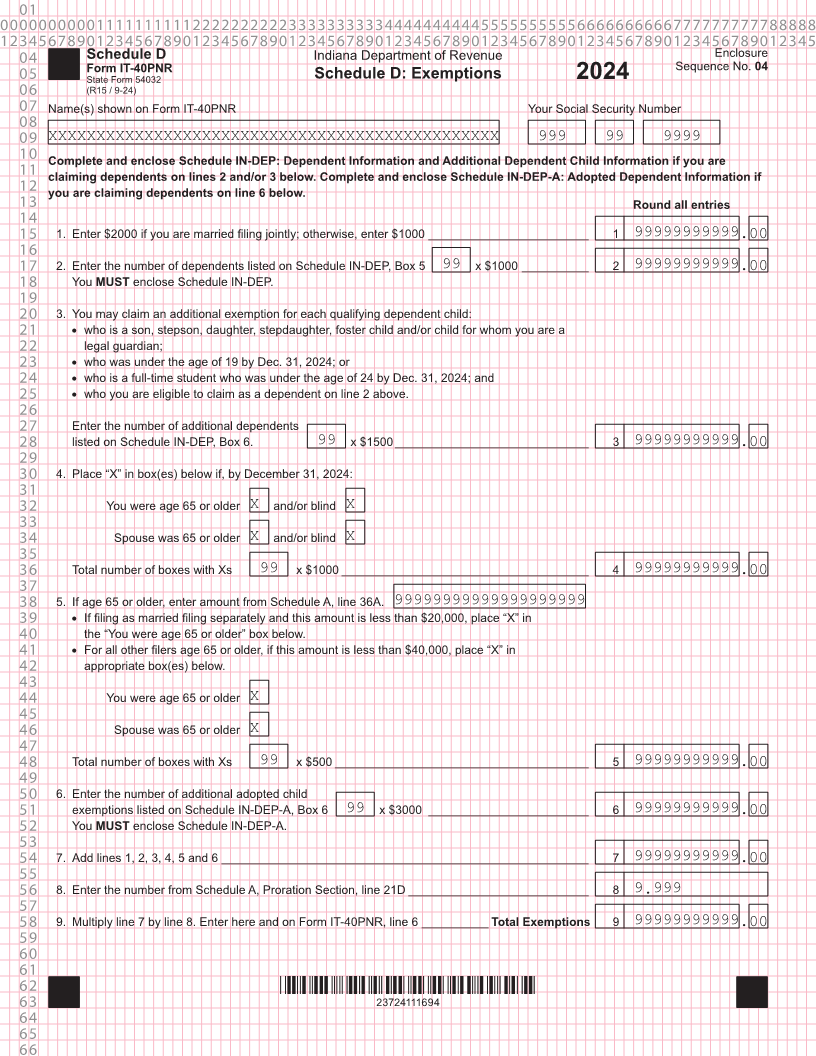
04 Schedule D Indiana Department of Revenue Enclosure
Form IT-40PNR Sequence No. 04
05 State Form 54032 Schedule D: Exemptions 2024
06 (R15 / 9-24)
07 Name(s) shown on Form IT-40PNR Your Social Security Number
08
09 XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX 999 99 9999
10 Complete and enclose Schedule IN-DEP: Dependent Information and Additional Dependent Child Information if you are
11 claiming dependents on lines 2 and/or 3 below. Complete and enclose Schedule IN-DEP-A: Adopted Dependent Information if
12 you are claiming dependents on line 6 below.
13 Round all entries
14
15 1. Enter $2000 if you are married filing jointly; otherwise, enter $1000 ________________________ 1 99999999999.00
16
17 2. Enter the number of dependents listed on Schedule IN-DEP, Box 5 99 x $1000 __________ 2 99999999999.00
18 You MUST enclose Schedule IN-DEP.
19
20 3. You may claim an additional exemption for each qualifying dependent child:
21 • who is a son, stepson, daughter, stepdaughter, foster child and/or child for whom you are a
22 legal guardian;
23 • who was under the age of 19 by Dec. 31, 2024; or
24 • who is a full-time student who was under the age of 24 by Dec. 31, 2024; and
25 • who you are eligible to claim as a dependent on line 2 above.
26
27 Enter the number of additional dependents
28 listed on Schedule IN-DEP, Box 6. 99 x $1500 _____________________________ 3 99999999999.00
29
30 4. Place “X” in box(es) below if, by December 31, 2024:
31
32 You were age 65 or older X and/or blind X
33
34 Spouse was 65 or older X and/or blind X
35
36 Total number of boxes with Xs 99 x $1000 _____________________________________ 4 99999999999.00
37
38 5. If age 65 or older, enter amount from Schedule A, line 36A. 99999999999999999999
39 • If filing as married filing separately and this amount is less than $20,000, place “X” in
40 the “You were age 65 or older” box below.
41 • For all other filers age 65 or older, if this amount is less than $40,000, place “X” in
42 appropriate box(es) below.
43
44 You were age 65 or older X
45
46 Spouse was 65 or older X
47
48 Total number of boxes with Xs 99 x $500 ______________________________________ 5 99999999999.00
49
50 6. Enter the number of additional adopted child
51 exemptions listed on Schedule IN-DEP-A, Box 6 99 x $3000 ________________________ 6 99999999999.00
52 You MUST enclose Schedule IN-DEP-A.
53
54 7. Add lines 1, 2, 3, 4, 5 and 6 _______________________________________________________ 7 99999999999.00
55
56 8. Enter the number from Schedule A, Proration Section, line 21D ___________________________ 8 9.999
57
58 9. Multiply line 7 by line 8. Enter here and on Form IT-40PNR, line 6 __________Total Exemptions 9 99999999999.00
59
60
61
62 *23724111694*
63 23724111694
64
65
66