Enlarge image
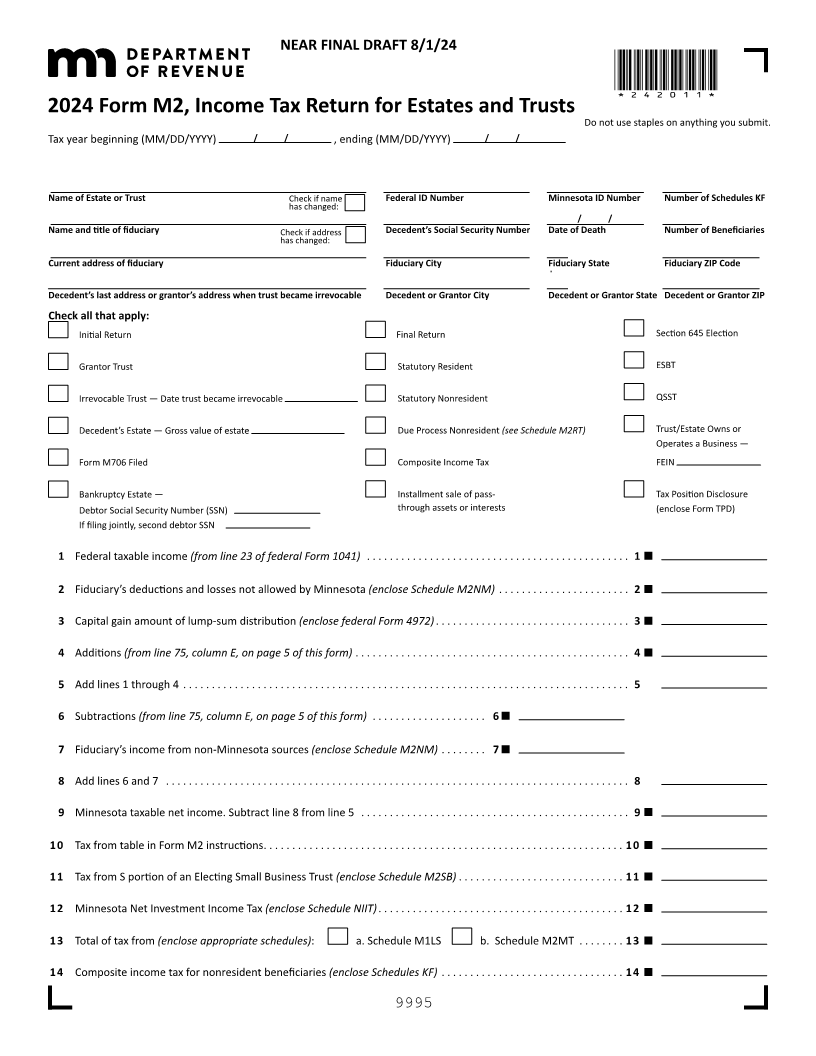
NEAR FINAL DRAFT 8/1/24
*242011*
2024 Form M2, Income Tax Return for Estates and Trusts
Do not use staples on anything you submit.
Tax year beginning (MM/DD/YYYY) / / , ending (MM/DD/YYYY) / /
Name of Estate or Trust Check if name Federal ID Number Minnesota ID Number Number of Schedules KF
has changed:
/ /
Name and title of fiduciary Check if address Decedent’s Social Security Number Date of Death Number of Beneficiaries
has changed:
Current address of fiduciary Fiduciary City Fiduciary State Fiduciary ZIP Code
Decedent’s last address or grantor’s address when trust became irrevocable Decedent or Grantor City Decedent or Grantor State Decedent or Grantor ZIP
Check all that apply:
Initial Return Final Return Section 645 Election
Grantor Trust Statutory Resident ESBT
Irrevocable Trust — Date trust became irrevocable Statutory Nonresident QSST
Decedent’s Estate — Gross value of estate Due Process Nonresident (see Schedule M2RT) Trust/Estate Owns or
Operates a Business —
Form M706 Filed Composite Income Tax FEIN
Bankruptcy Estate — Installment sale of pass- Tax Position Disclosure
Debtor Social Security Number (SSN) through assets or interests (enclose Form TPD)
If filing jointly, second debtor SSN
1 Federal taxable income (from line 23 of federal Form 1041) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
2 Fiduciary’s deductions and losses not allowed by Minnesota (enclose Schedule M2NM) . . . . . . . . . . . . . . . . . . . . . . . 2
3 Capital gain amount of lump-sum distribution (enclose federal Form 4972) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
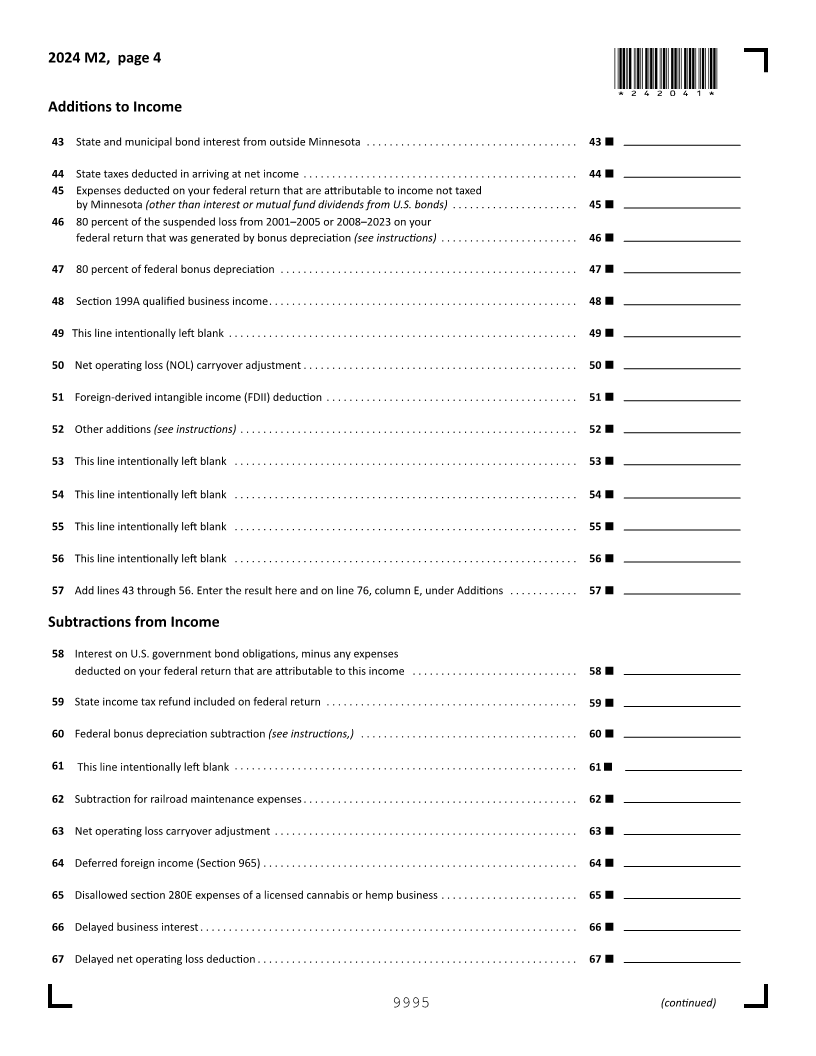
4 Additions (from line 75, column E, on page 5 of this form) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
5 Add lines 1 through 4 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
6 Subtractions (from line 75, column E, on page 5 of this form) . . . . . . . . . . . . . . . . . . . . 6
7Fiduciary’s from income non-Minnesota sources (enclose Schedule M2NM) . . . . . . . . 7
8 Add lines 6 and 7 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
9 Minnesota taxable net income. Subtract line 8 from line 5 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
10 Tax from table in Form M2 instructions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
11 Tax from S portion of an Electing Small Business Trust (enclose Schedule M2SB) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
12 Minnesota Net Investment Income Tax (enclose Schedule NIIT) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
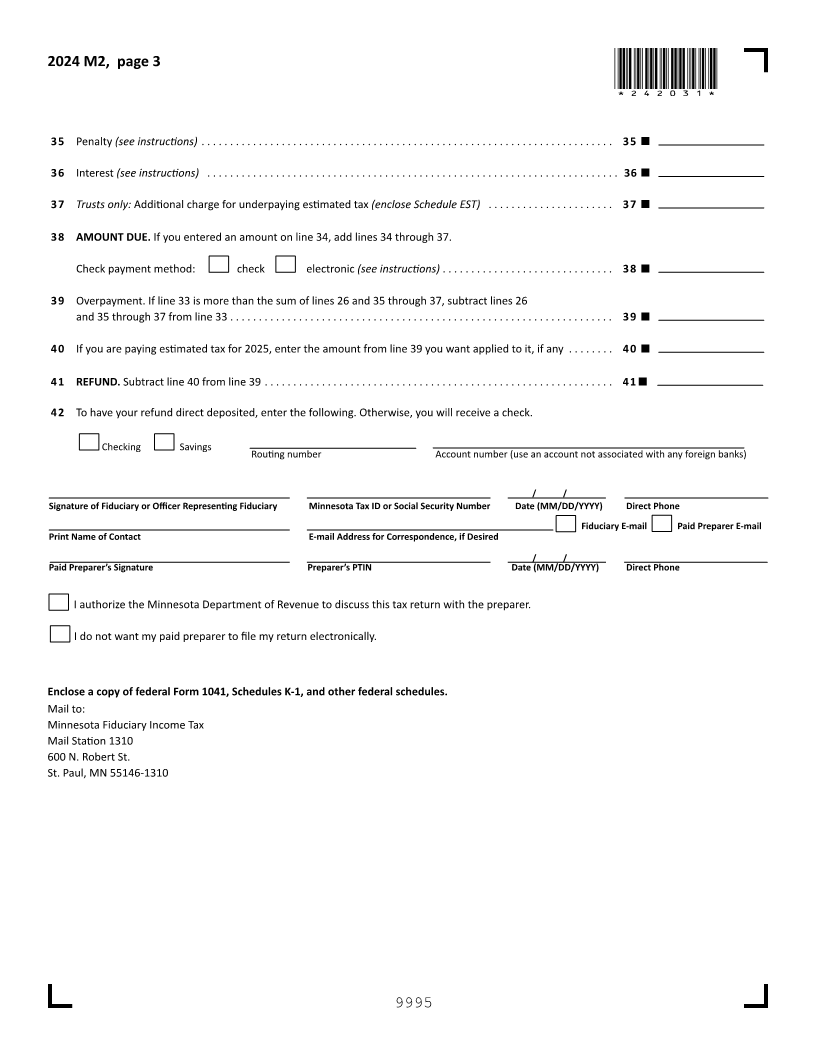
13 Total of tax from (enclose appropriate schedules): a. Schedule M1LS b. Schedule M2MT . . . . . . . . 13
14 Composite income tax for nonresident beneficiaries (enclose Schedules KF) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
9995