Enlarge image
NEAR FINAL 8/1/24
*226281*
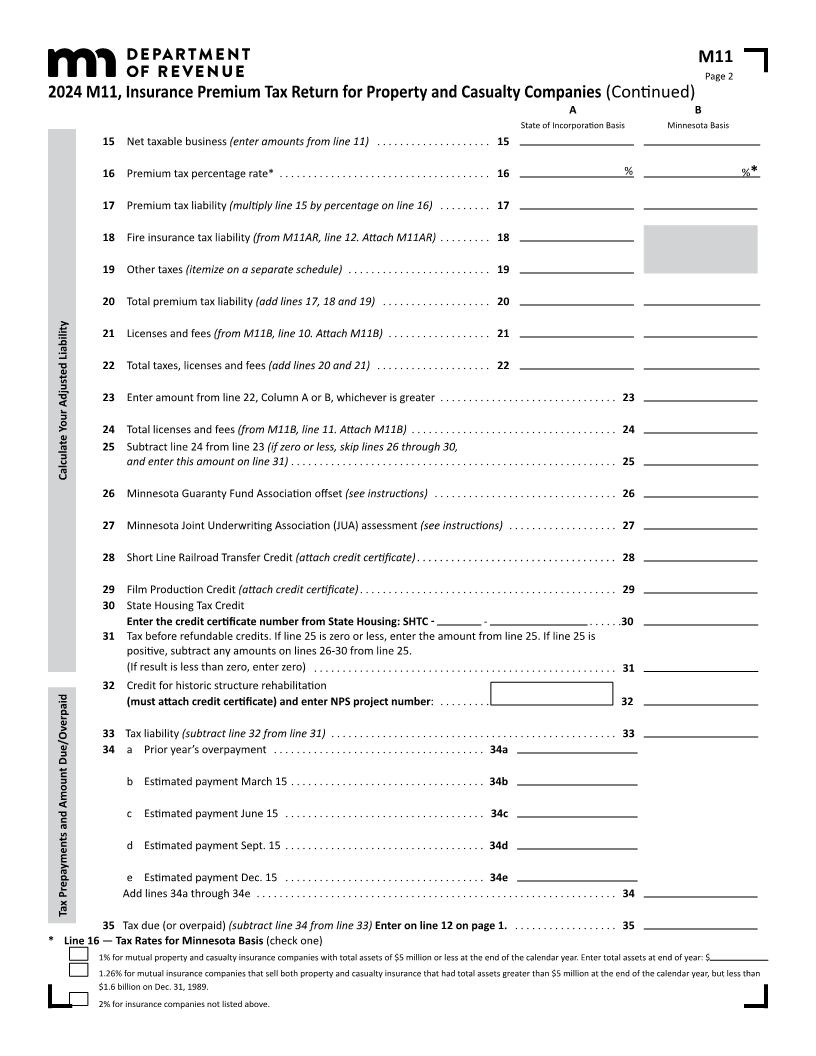
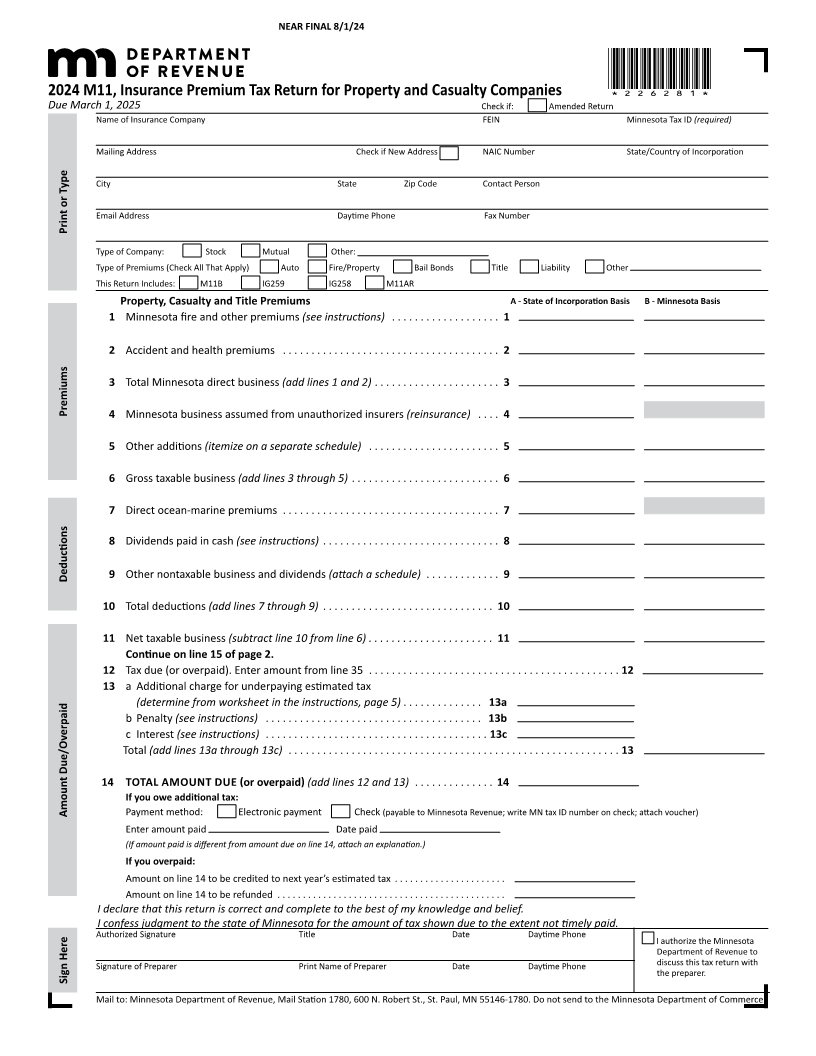
2024 M11, Insurance Premium Tax Return for Property and Casualty Companies
Due March 1, 2025 Check if: Amended Return
Name of Insurance Company FEIN Minnesota Tax ID (required)
Mailing Address Check if New Address NAIC Number State/Country of Incorporation
City State Zip Code Contact Person
Email Address Daytime Phone Fax Number
Print or Type
Type of Company: Stock Mutual Other:
Type of Premiums (Check All That Apply) Auto Fire/Property Bail Bonds Title Liability Other
This Return Includes: M11B IG259 IG258 M11AR
Property, Casualty and Title Premiums A - State of Incorporation Basis B - Minnesota Basis
1 Minnesota fire and other premiums (see instructions) . . . . . . . . . . . . . . . . . . . 1
2 Accident and health premiums . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
3 Total Minnesota direct business (add lines 1 and 2) . . . . . . . . . . . . . . . . . . . . . . 3
Premiums 4 Minnesota business assumed from unauthorized insurers (reinsurance) . . . . 4
5 Other additions (itemize on a separate schedule) . . . . . . . . . . . . . . . . . . . . . . . 5
6 Gross taxable business (add lines 3 through 5) . . . . . . . . . . . . . . . . . . . . . . . . . . 6
7 Direct ocean-marine premiums . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
8 Dividends paid in cash (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Deductions 9 Other nontaxable business and dividends (attach a schedule) . . . . . . . . . . . . . 9
10 Total deductions (add lines 7 through 9) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
11 Net taxable business (subtract line 10 from line 6) . . . . . . . . . . . . . . . . . . . . . . 11
Continue on line 15 of page 2.
12 Tax due (or overpaid) . Enter amount from line 35 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
13 a Additional charge for underpaying estimated tax
(determine from worksheet in the instructions, page 5) . . . . . . . . . . . . . . 13a
b Penalty (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13b
c Interest (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13c
Total (add lines 13a through 13c) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
14 TOTAL AMOUNT DUE (or overpaid ) (add lines 12 and 13) . . . . . . . . . . . . . . 14
If you owe additional tax:
Amount Due/Overpaid Payment method: Electronic payment Check (payable to Minnesota Revenue; write MN tax ID number on check; attach voucher)
Enter amount paid Date paid
(If amount paid is different from amount due on line 14, attach an explanation.)
If you overpaid:
Amount on line 14 to be credited to next year’s estimated tax . . . . . . . . . . . . . . . . . . . . . .
Amount on line 14 to be refunded . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
I declare that this return is correct and complete to the best of my knowledge and belief.
I confess judgment to the state of Minnesota for the amount of tax shown due to the extent not timely paid.
Authorized Signature Title Date Daytime Phone
I authorize the Minnesota
Department of Revenue to
Signature of Preparer Print Name of Preparer Date Daytime Phone discuss this tax return with
Sign Here the preparer .
Mail to: Minnesota Department of Revenue, Mail Station 1780, 600 N. Robert St., St. Paul, MN 55146-1780. Do not send to the Minnesota Department of Commerce.