Enlarge image
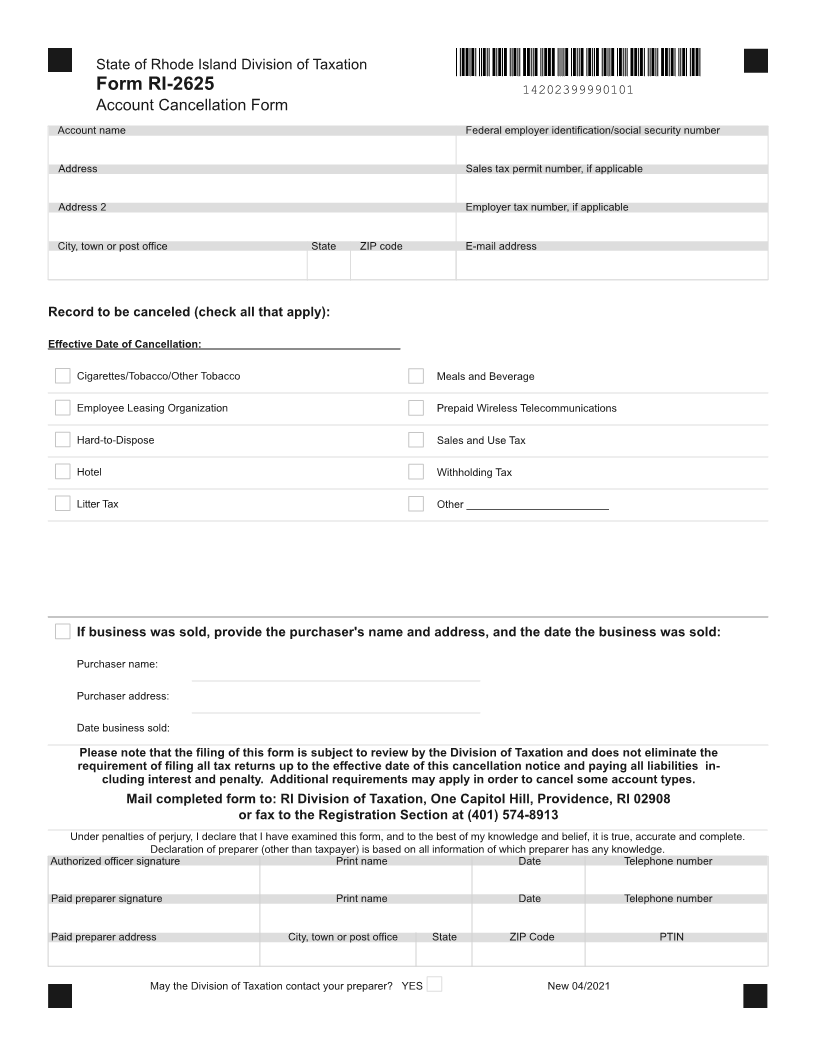
State of Rhode Island Division of Taxation
Form RI-2625
14202399990101
Account Cancellation Form
Account name Federal employer identification/social security number
Address Sales tax permit number, if applicable
Address 2 Employer tax number, if applicable
City, town or post office State ZIP code E-mail address
Record to be canceled (check all that apply):
Effective Date of Cancellation:
Cigarettes/Tobacco/Other Tobacco Meals and Beverage
Employee Leasing Organization Prepaid Wireless Telecommunications
Hard-to-Dispose Sales and Use Tax
Hotel Withholding Tax
Litter Tax Other ________________________
If business was sold, provide the purchaser's name and address, and the date the business was sold:
Purchaser name:
Purchaser address:
Date business sold:
Please note that the filing of this form is subject to review by the Division of Taxation and does not eliminate the
requirement of filing all tax returns up to the effective date of this cancellation notice and paying all liabilities in-
cluding interest and penalty. Additional requirements may apply in order to cancel some account types.
Mail completed form to: RI Division of Taxation, One Capitol Hill, Providence, RI 02908
or fax to the Registration Section at (401) 574-8913
Under penalties of perjury, I declare that I have examined this form, and to the best of my knowledge and belief, it is true, accurate and complete.
Declaration of preparer (other than taxpayer) is based on all information of which preparer has any knowledge.
Authorized officer signature Print name Date Telephone number
Paid preparer signature Print name Date Telephone number
Paid preparer address City, town or post office State ZIP Code PTIN
May the Division of Taxation contact your preparer? YES New 04/2021