Enlarge image
OMB Control No. 1205-0371
U.S. Department of Labor Expiration Date: May 31, 2026
Employment and Training Administration
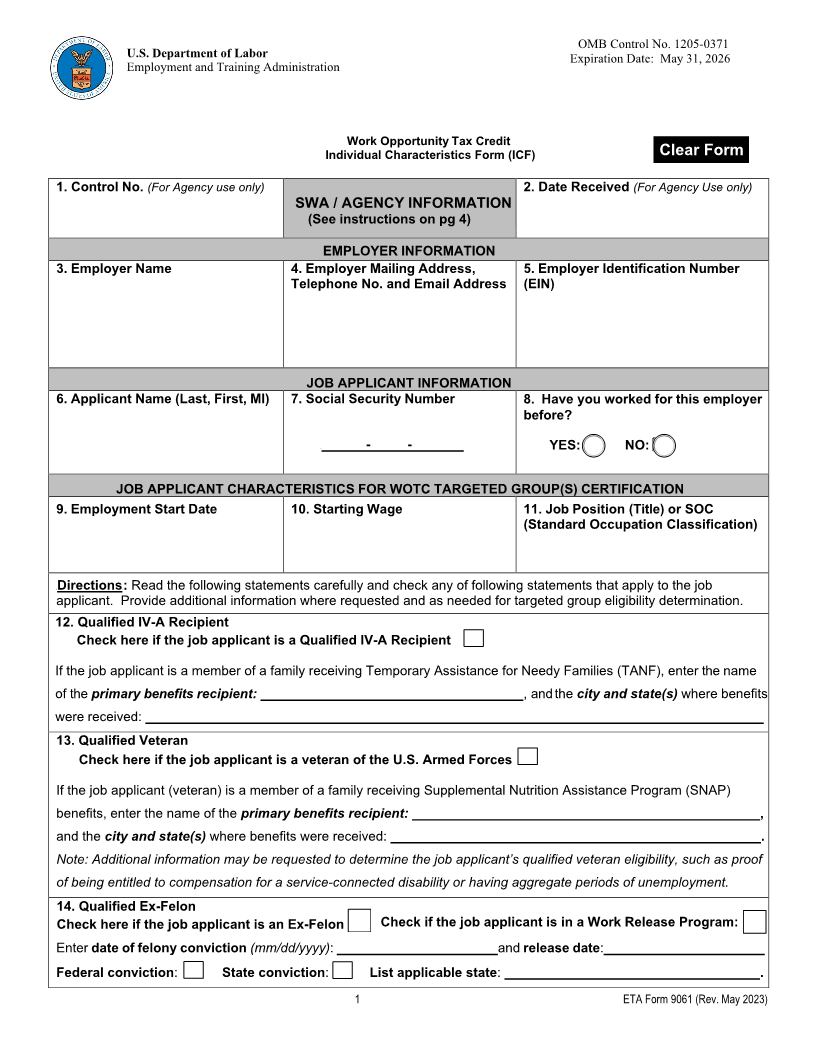
Work Opportunity Tax Credit
Individual Characteristics Form (ICF) Clear Form
1. Control No. (For Agency use only) 2. Date Received (For Agency Use only)
SWA / AGENCY INFORMATION
(See instructions on pg 4)
EMPLOYER INFORMATION
3. Employer Name 4. Employer Mailing Address, 5. Employer Identification Number
Telephone No. and Email Address (EIN)
JOB APPLICANT INFORMATION
6. Applicant Name (Last, First, MI) 7. Social Security Number 8. Have you worked for this employer
before?
U - - YES: NO:
JOB APPLICANT CHARACTERISTICS FOR WOTC TARGETED GROUP(S) CERTIFICATION
9. Employment Start Date 10. Starting Wage 11. Job Position (Title) or SOC
(Standard Occupation Classification)
UDirections:U Read the following statements carefully and check any of following statements that apply to the job
applicant. Provide additional information where requested and as needed for targeted group eligibility determination.
12. Qualified IV-A Recipient
Check here if the job applicant is a Qualified IV-A Recipient
If the job applicant is a member of a family receiving Temporary Assistance for Needy Families (TANF), enter the name
of the primary benefits recipient: , and the city and state(s) where benefits
were received:
13. Qualified Veteran
Check here if the job applicant is a veteran of the U.S. Armed Forces
If the job applicant (veteran) is a member of a family receiving Supplemental Nutrition Assistance Program (SNAP)
benefits, enter the name of the primary benefits recipient: ,
and the city and state(s) where benefits were received: .
Note: Additional information may be requested to determine the job applicant’s qualified veteran eligibility, such as proof
of being entitled to compensation for a service-connected disability or having aggregate periods of unemployment.
14. Qualified Ex-Felon
Check if the job applicant is in a Work Release Program:
Check here if the job applicant is an Ex-Felon
Enterdate of felony conviction(mm/dd/yyyy): andrelease date :
Federal conviction: State conviction: List applicable state : .
1 ETA Form 9061 (Rev. May 2023)