- 2 -
Enlarge image
|
Steps to Complete this Survey
This survey requires employers to provide information about work-related injuries and illnesses based upon the
information you have maintained for Calendar Year 2022 on your Occupational Safety and Health Administration
(OSHA) Forms for Recording Work-Related Injuries and Illnesses. Copies of these forms were sent to you in late 2021.
Under Public Law 91-596, all establishments that receive this mandatory survey must complete and return it within 30
days, even if they had no work-related injuries and illnesses during 2022. The instructions below outline the steps to
complete the survey regardless of whether or not your establishment had injuries or illnesses in 2022.
Step 1: Complete this survey only for the establishment(s) noted on the front cover under “Report for this Location.” If
you are unsure, please call the number(s) listed on the front of this form in the “For Help Call:” section.
Step 2: Check “Your Company Address” printed on the front cover. Make any necessary corrections directly on the
front cover.
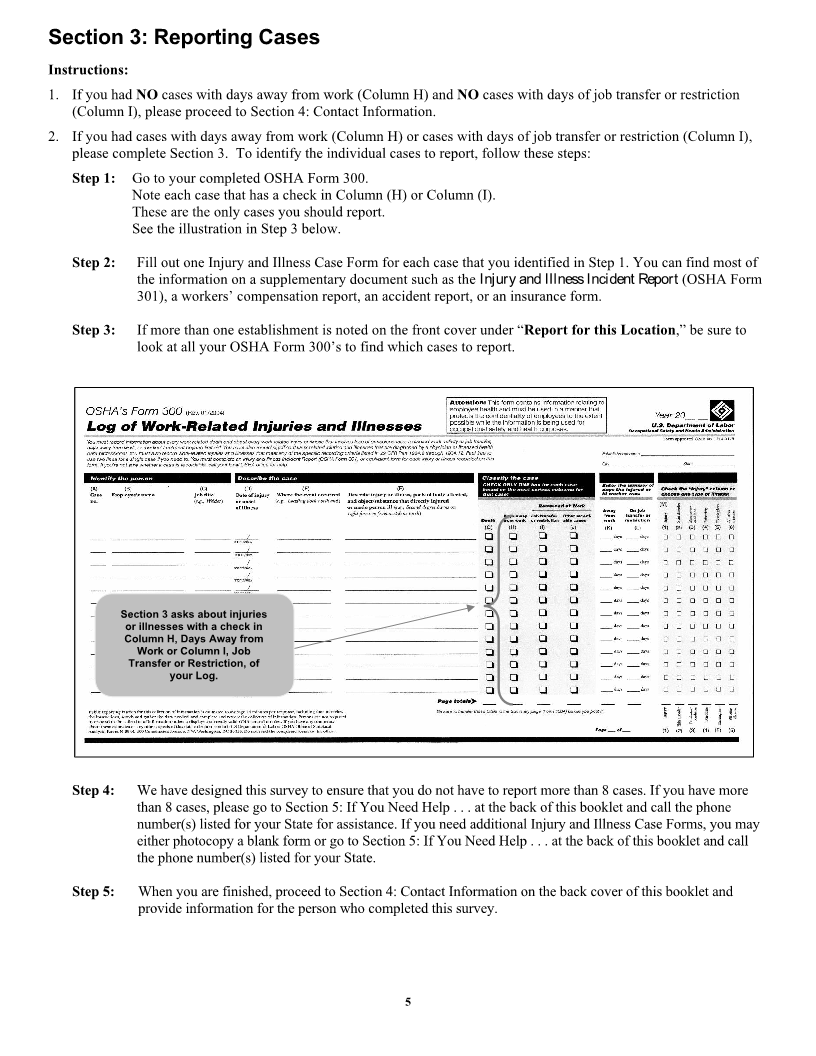
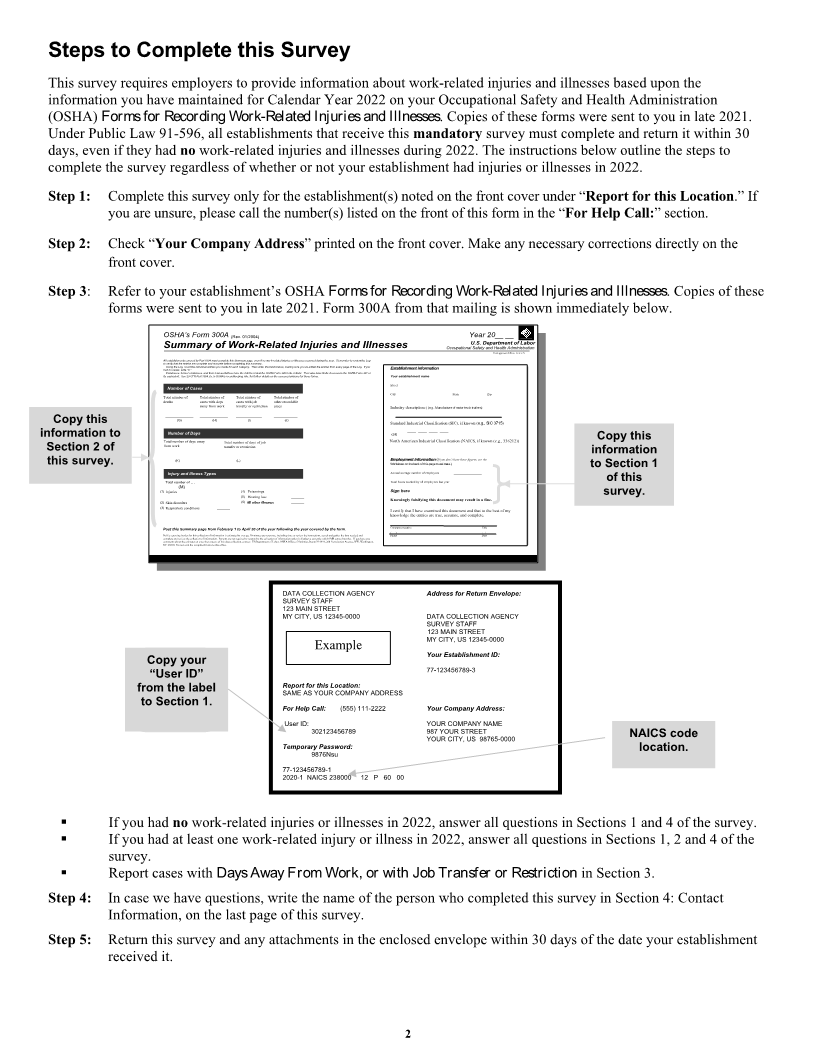
Step 3: Refer to your establishment’s OSHA Forms for Recording Work-Related Injuries and Illnesses. Copies of these
forms were sent to you in late 2021. Form 300A from that mailing is shown immediately below.
Summary of Work-Related Injuries and Illnesses
OSHA’s Form 300A (Rev. 01/2004) OccupationalYear 20__SafetyU.S.__ Departmentand HealthForm approvedAdministrationOMBofno. 1218-0176Labor
itstohadAllEmployees,Usingverifyequivalent. establishmentsnothecases,thatLog,theformerwriteSeecountentriescovered29“0.”employees,theCFRareindividualbycompletePartPartand1904.35,1904entriestheirandmustrepresentativesaccurateinyouOSHA’scompletemadebeforerecordkeepingforthiseachhavecompletingSummarycategory. the rightrule,thispage,toThenforsummaryreviewfurtherevenwrite theifthedetailsnoOSHAwortotals. onk-relatedFormbelow,the access300injuriesmakinginprovisionsitsorentirety. sureillnessesyou’veforTheyoccurredtheseaddedalsoforms. havetheduringentrieslimitethedfromyear. accesseveryRemembertopagethe OSHAoftothereviewFormLog. 301theIf you Logor EstablishmentYourEstablishment establishment informationinformationname ______________________________________
Number of Cases Street ____________________________________________________
Total number of Total number of City _______________________ State ____________ Zip ________
Totaldeathsnumber of Totalcasesaway withfromnumberdaysworkof transfercases withor restrictionjob casesother recordable Industry description ( (e.g., Manufacture of motor truck trailers)
Copy this
Number of Days
information to _____________ (G) _____________ (H) (I)____________ ___________ (J) North Standard OR AmericanIndustrial____ ____ IndustrialClassification____ Classification____(SIC), if(NAICS,known (if knowne.g., SIC(e.g.,3715336212))) Copy this
Section 2 of fromTotalworknumber of days away Totaltransfernumberor restrictionof days of job ____ ____ ____ ____ ____ ____ information
this survey. _____________ (K) (L)______________ EmploymentWorksheetEmployment on the back informationinformationof this page to (estimate.)If you don’t have these figures, see the to Section 1
Injury and Illness Types Annual average number of employees _____________
Total hours worked by all employees last year _____________ of this
(1) (M)TotalInjuries number of … ______ (5)(4) PoisoningsHearing loss ____________ Sign here survey.
All other illnesses Knowingly falsifying this document may result in a fine.
(2) (3) RespiratorySkin disordersconditions ____________ (6) All other illnesses ______ Iknowledgecertify thattheI haveentriesexaminedare true,thisaccurate,documentandandcomplete.that to the best of my
Company executive Title
PublicPostreportingthis Summaryburden for this collectionpage fromof informationFebruaryis estimated1 totoAprilaverage 5030minutesof theperyearresponse,followingincluding timetheto reviewyearthecoveredinstructions, searchby theand gatherform.the data needed, and ( Phone ) Date/ /
completecommentsDC 20210. andaboutDoreviewnotthesendestimatesthethecollectioncompletedor anyofotherinformation. formsaspectsto thisofPersonsoffice.this dataarecollection,not requiredcontact: to respondUS Departmentto the collectionof Labor,of informationOSHA Officeunlessof Statistics,it displaysRooma currentlyN-3644,valid200OMBConstitutioncontrol number. Avenue,IfNW,youWashington,have any
DATA COLLECTION AGENCY Address for Return Envelope:
SURVEY STAFF
123 MAIN STREET
MY CITY, US 12345-0000 DATA COLLECTION AGENCY
SURVEY STAFF
123 MAIN STREET
MY CITY, US 12345-0000
Example Your Establishment ID:
Copy your
“User ID” 77-123456789-3
from the label Report for this Location:
SAME AS YOUR COMPANY ADDRESS
to Section 1. For Help Call: (555) 111-2222 Your Company Address:
User ID: YOUR COMPANY NAME
302123456789 987 YOUR STREET
YOUR CITY, US 98765-0000 NAICS code
Temporary Password:
9876Nsu location.
77-123456789-1
2020-1 NAICS 238000 12 P 60 00
▪ If you had no work-related injuries or illnesses in 2022, answer all questions in Sections 1 and 4 of the survey.
▪ If you had at least one work-related injury or illness in 2022, answer all questions in Sections 1, 2 and 4 of the
survey.
▪ Report cases with Days Away From Work, or with Job Transfer or Restriction in Section 3.
Step 4: In case we have questions, write the name of the person who completed this survey in Section 4: Contact
Information, on the last page of this survey.
Step 5: Return this survey and any attachments in the enclosed envelope within 30 days of the date your establishment
received it.
2
|