Enlarge image
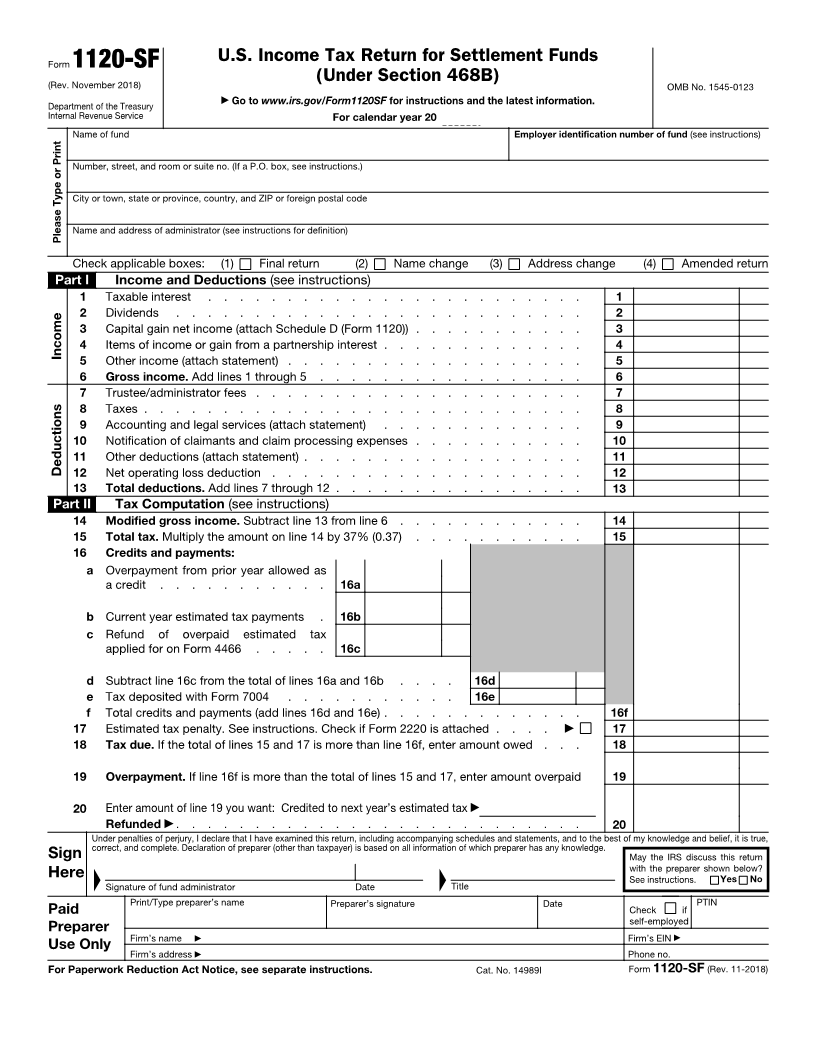
U.S. Income Tax Return for Settlement Funds
Form 1120-SF
(Rev. November 2018) (Under Section 468B) OMB No. 1545-0123
▶
Department of the Treasury Go to www.irs.gov/Form1120SF for instructions and the latest information.
Internal Revenue Service For calendar year 20
Name of fund Employer identification number of fund (see instructions)
Number, street, and room or suite no. (If a P.O. box, see instructions.)
City or town, state or province, country, and ZIP or foreign postal code
Name and address of administrator (see instructions for definition)
Please Type or Print
Check applicable boxes: (1) Final return (2) Name change (3) Address change (4) Amended return
Part I Income and Deductions (see instructions)
1 Taxable interest . . . . . . . . . . . . . . . . . . . . . . . . 1
2 Dividends . . . . . . . . . . . . . . . . . . . . . . . . . . 2
3 Capital gain net income (attach Schedule D (Form 1120)) . . . . . . . . . . . 3
4 Items of income or gain from a partnership interest . . . . . . . . . . . . . 4
Income
5 Other income (attach statement) . . . . . . . . . . . . . . . . . . . 5
6 Gross income. Add lines 1 through 5 . . . . . . . . . . . . . . . . . 6
7 Trustee/administrator fees . . . . . . . . . . . . . . . . . . . . . 7
8 Taxes . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
9 Accounting and legal services (attach statement) . . . . . . . . . . . . . 9
10 Notification of claimants and claim processing expenses . . . . . . . . . . . 10
11 Other deductions (attach statement) . . . . . . . . . . . . . . . . . . 11
Deductions 12 Net operating loss deduction . . . . . . . . . . . . . . . . . . . . 12
13 Total deductions. Add lines 7 through 12 . . . . . . . . . . . . . . . . 13
Part II Tax Computation (see instructions)
14 Modified gross income. Subtract line 13 from line 6 . . . . . . . . . . . . 14
15 Total tax. Multiply the amount on line 14 by 37% (0.37) . . . . . . . . . . . 15
16 Credits and payments:
a Overpayment from prior year allowed as
a credit . . . . . . . . . . . 16a
b Current year estimated tax payments . 16b
c Refund of overpaid estimated tax
applied for on Form 4466 . . . . . 16c
d Subtract line 16c from the total of lines 16a and 16b . . . . 16d
e Tax deposited with Form 7004 . . . . . . . . . . . 16e
f Total credits and payments (add lines 16d and 16e) . . . . . . . . . . . . . 16f
17 Estimated tax penalty. See instructions. Check if Form 2220 is attached . . . . ▶ 17
18 Tax due. If the total of lines 15 and 17 is more than line 16f, enter amount owed . . . 18
19 Overpayment. If line 16f is more than the total of lines 15 and 17, enter amount overpaid 19
20 Enter amount of line 19 you want: Credited to next year’s estimated tax ▶
Refunded ▶ . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Under penalties of perjury, I declare that I have examined this return, including accompanying schedules and statements, and to the best of my knowledge and belief, it is true,
correct, and complete. Declaration of preparer (other than taxpayer) is based on all information of which preparer has any knowledge.
Sign ▲ ▲ May the IRS discuss this return
with the preparer shown below?
Here See instructions. Yes No
Signature of fund administrator Date Title
Print/Type preparer’s name Preparer’s signature Date PTIN
Paid Check if
self-employed
Preparer ▶
Firm’s name ▶ Firm’s EIN
Firm’s address
Use Only ▶ Phone no.
For Paperwork Reduction Act Notice, see separate instructions. Cat. No. 14989I Form 1120-SF (Rev. 11-2018)