- 5 -
Enlarge image
|
Form 5300 (Rev. 1-2017) Page 3
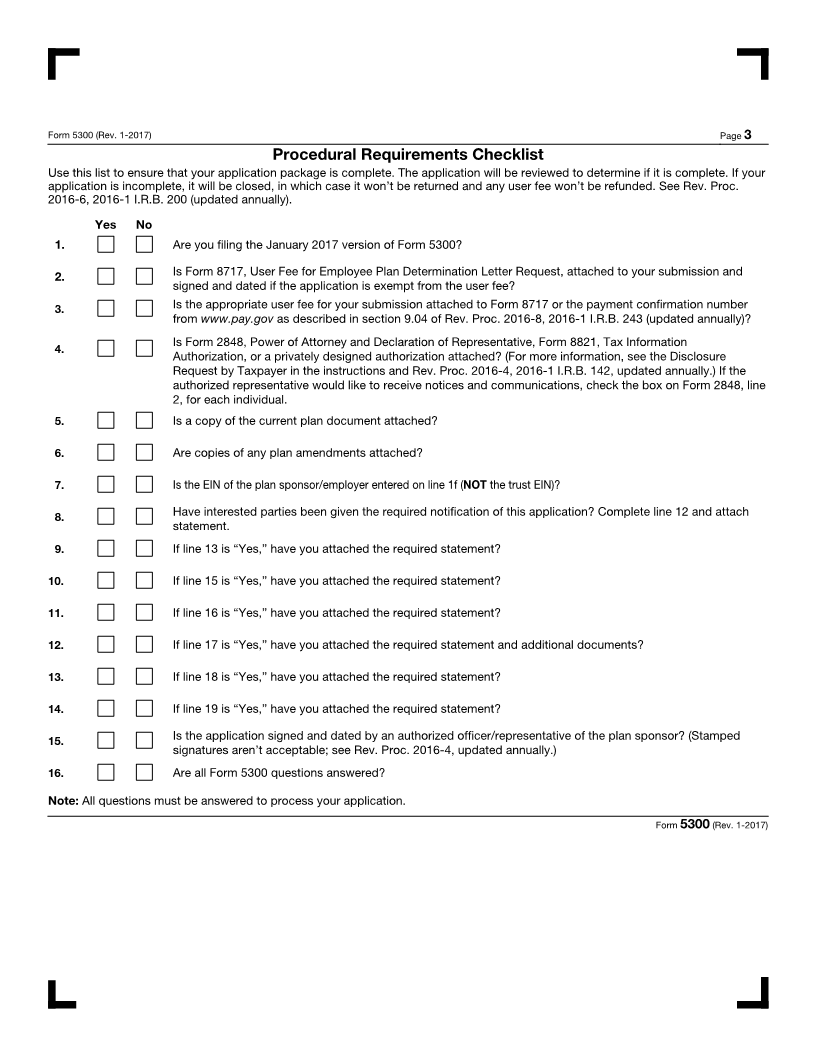
Procedural Requirements Checklist
Use this list to ensure that your application package is complete. The application will be reviewed to determine if it is complete. If your
application is incomplete, it will be closed, in which case it won’t be returned and any user fee won’t be refunded. See Rev. Proc.
2016-6, 2016-1 I.R.B. 200 (updated annually).
Yes No
1. Are you filing the January 2017 version of Form 5300?
2. Is Form 8717, User Fee for Employee Plan Determination Letter Request, attached to your submission and
signed and dated if the application is exempt from the user fee?
3. Is the appropriate user fee for your submission attached to Form 8717 or the payment confirmation number
from www.pay.gov as described in section 9.04 of Rev. Proc. 2016-8, 2016-1 I.R.B. 243 (updated annually)?
Is Form 2848, Power of Attorney and Declaration of Representative, Form 8821, Tax Information
4.
Authorization, or a privately designed authorization attached? (For more information, see the Disclosure
Request by Taxpayer in the instructions and Rev. Proc. 2016-4, 2016-1 I.R.B. 142, updated annually.) If the
authorized representative would like to receive notices and communications, check the box on Form 2848, line
2, for each individual.
5. Is a copy of the current plan document attached?
6. Are copies of any plan amendments attached?
7. Is the EIN of the plan sponsor/employer entered on line 1f (NOT the trust EIN)?
8. Have interested parties been given the required notification of this application? Complete line 12 and attach
statement.
9. If line 13 is “Yes,” have you attached the required statement?
10. If line 15 is “Yes,” have you attached the required statement?
11. If line 16 is “Yes,” have you attached the required statement?
12. If line 17 is “Yes,” have you attached the required statement and additional documents?
13. If line 18 is “Yes,” have you attached the required statement?
14. If line 19 is “Yes,” have you attached the required statement?
15. Is the application signed and dated by an authorized officer/representative of the plan sponsor? (Stamped
signatures aren’t acceptable; see Rev. Proc. 2016-4, updated annually.)
16. Are all Form 5300 questions answered?
Note: All questions must be answered to process your application.
Form 5300 (Rev. 1-2017)
|