Enlarge image
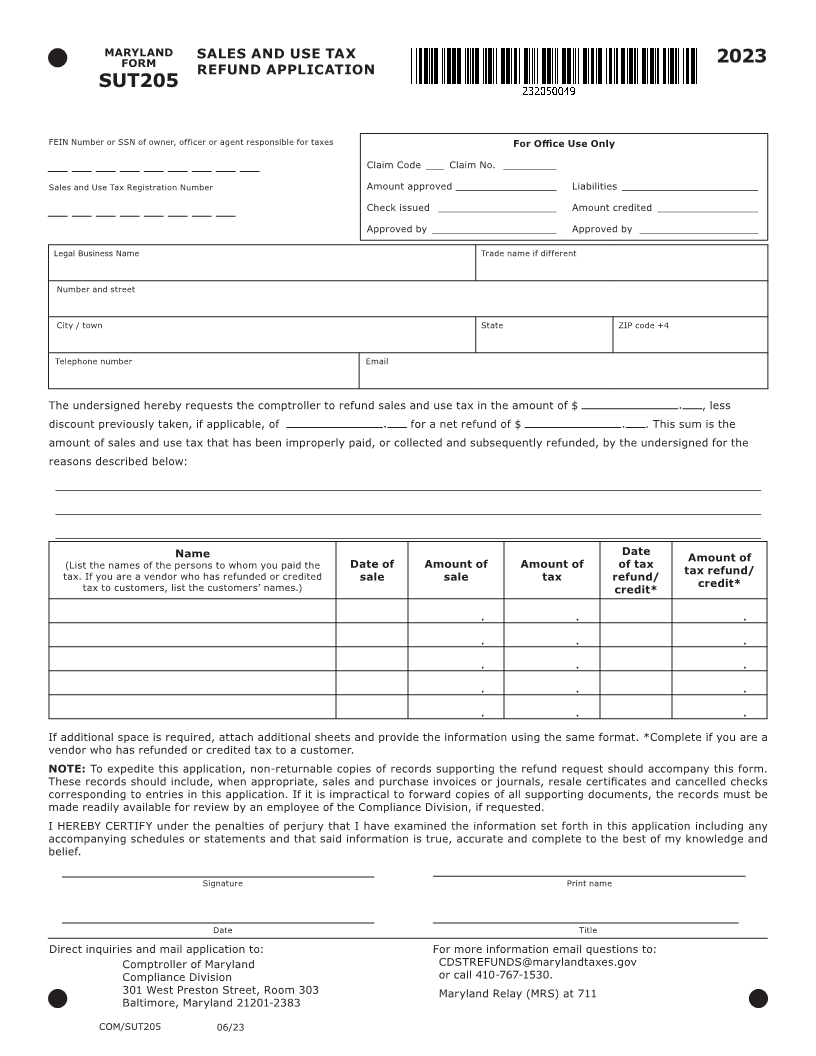
MARYLAND SALES AND USE TAX 2023
FORM
REFUND APPLICATION
SUT205
FEIN Number or SSN of owner, officer or agent responsible for taxes For Office Use Only
Claim Code ___ Claim No. _________
Sales and Use Tax Registration Number Amount approved _________________ Liabilities _______________________
Check issued ____________________ Amount credited _________________
Approved by _____________________ Approved by ____________________
Legal Business Name Trade name if different
Number and street
City / town State ZIP code +4
Telephone number Email
The undersigned hereby requests the comptroller to refund sales and use tax in the amount of $ , less
discount previously taken, if applicable, of for a net refund of $ . This sum is the
amount of sales and use tax that has been improperly paid, or collected and subsequently refunded, by the undersigned for the
reasons described below:
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
Name Date Amount of
(List the names of the persons to whom you paid the Date of Amount of Amount of of tax tax refund/
tax. If you are a vendor who has refunded or credited sale sale tax refund/ credit*
tax to customers, list the customers’ names.) credit*
. . .
. . .
. . .
. . .
. . .
If additional space is required, attach additional sheets and provide the information using the same format. *Complete if you are a
vendor who has refunded or credited tax to a customer.
NOTE: To expedite this application, non-returnable copies of records supporting the refund request should accompany this form.
These records should include, when appropriate, sales and purchase invoices or journals, resale certificates and cancelled checks
corresponding to entries in this application. If it is impractical to forward copies of all supporting documents, the records must be
made readily available for review by an employee of the Compliance Division, if requested.
I HEREBY CERTIFY under the penalties of perjury that I have examined the information set forth in this application including any
accompanying schedules or statements and that said information is true, accurate and complete to the best of my knowledge and
belief.
Signature Print name
Date Title
Direct inquiries and mail application to: For more information email questions to:
Comptroller of Maryland CDSTREFUNDS@marylandtaxes.gov
Compliance Division or call 410-767-1530.
301 West Preston Street, Room 303 Maryland Relay (MRS) at 711
Baltimore, Maryland 21201-2383
COM/SUT205 06/23