Enlarge image
The form you are looking for begins on the next page of this file. Before viewing it, please see
the important update information below.
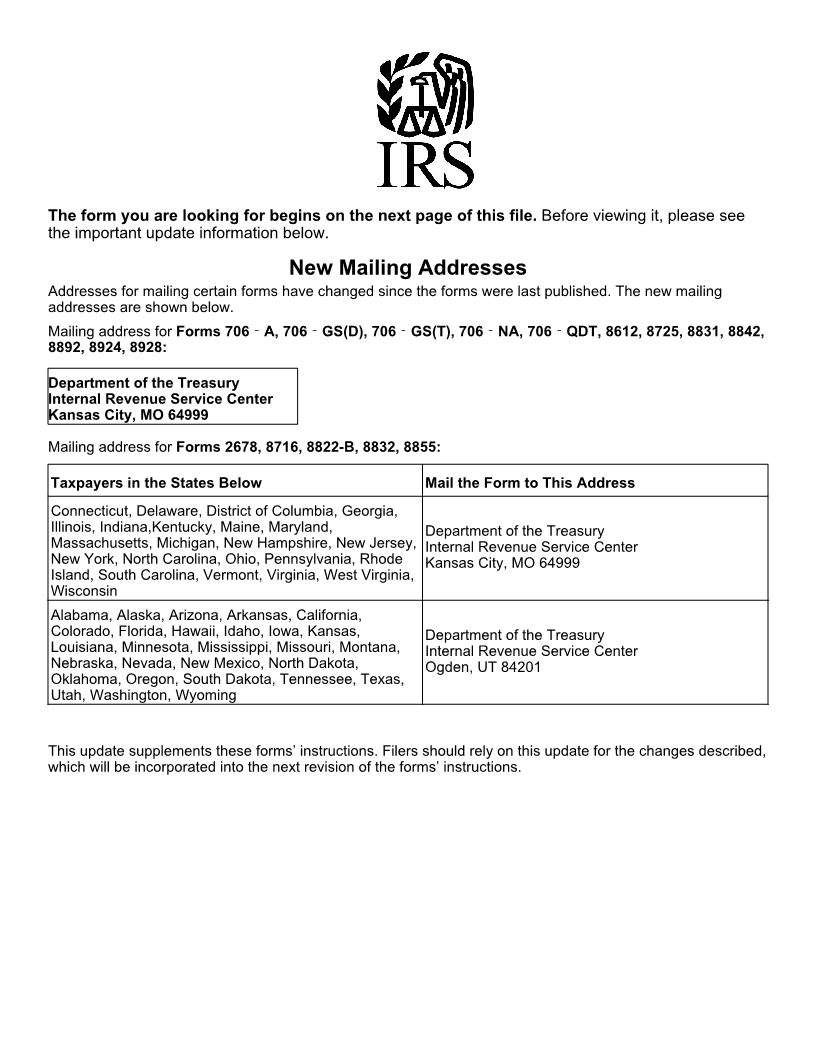
New Mailing Addresses
Addresses for mailing certain forms have changed since the forms were last published. The new mailing
addresses are shown below.
Mailing address for Forms 706‐A, 706‐GS(D), 706‐GS(T), 706‐NA, 706‐QDT, 8612, 8725, 8831, 8842,
8892, 8924, 8928:
Department of the Treasury
Internal Revenue Service Center
Kansas City, MO 64999
Mailing address for Forms 2678, 8716, 8822-B, 8832, 8855:
Taxpayers in the States Below Mail the Form to This Address
Connecticut, Delaware, District of Columbia, Georgia,
Illinois, Indiana,Kentucky, Maine, Maryland, Department of the Treasury
Massachusetts, Michigan, New Hampshire, New Jersey, Internal Revenue Service Center
New York, North Carolina, Ohio, Pennsylvania, Rhode Kansas City, MO 64999
Island, South Carolina, Vermont, Virginia, West Virginia,
Wisconsin
Alabama, Alaska, Arizona, Arkansas, California,
Colorado, Florida, Hawaii, Idaho, Iowa, Kansas, Department of the Treasury
Louisiana, Minnesota, Mississippi, Missouri, Montana, Internal Revenue Service Center
Nebraska, Nevada, New Mexico, North Dakota, Ogden, UT 84201
Oklahoma, Oregon, South Dakota, Tennessee, Texas,
Utah, Washington, Wyoming
This update supplements these forms’ instructions. Filers should rely on this update for the changes described,
which will be incorporated into the next revision of the forms’ instructions.