Enlarge image
Mail completed form to:
NH Attorney General’s Office
Attn: Charitable Trusts Unit
One Granite Place South
Concord, NH 03301
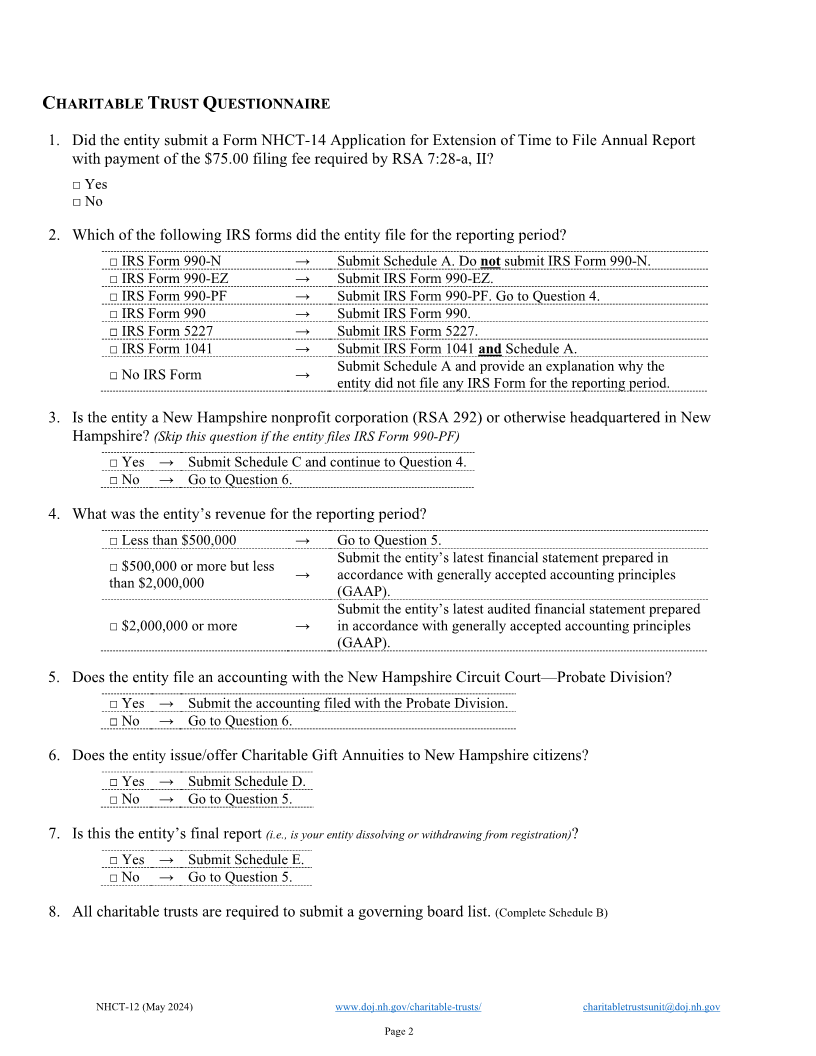
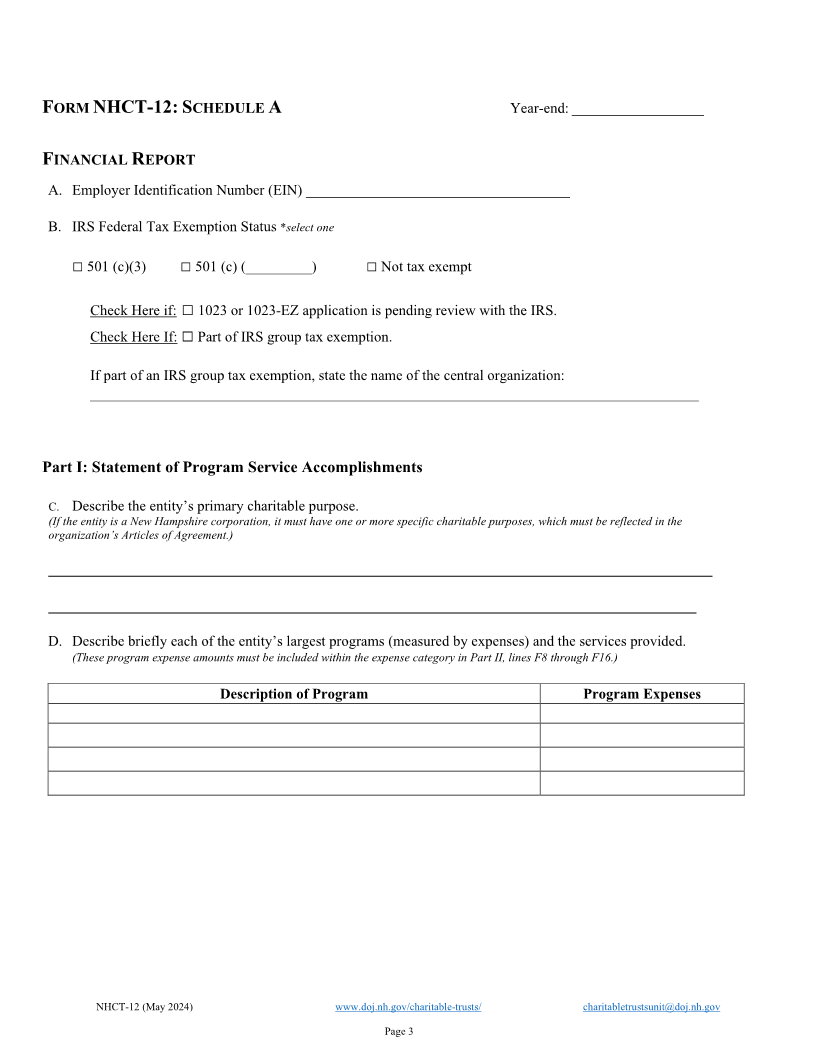
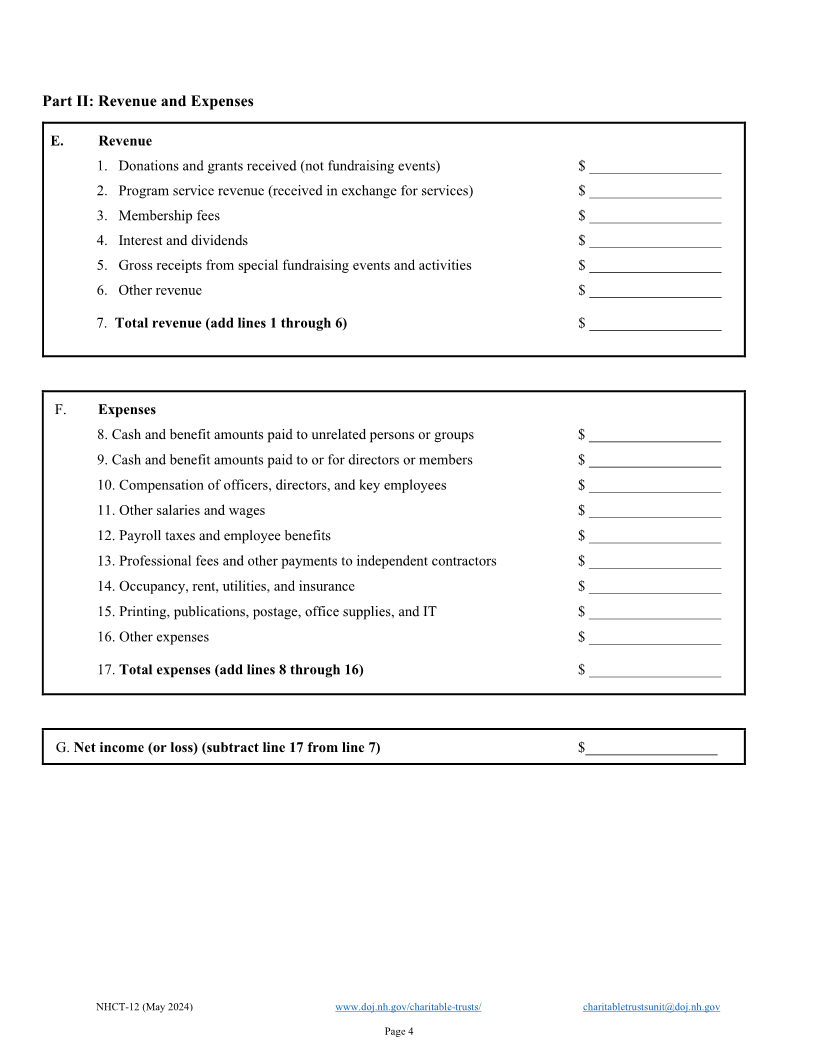
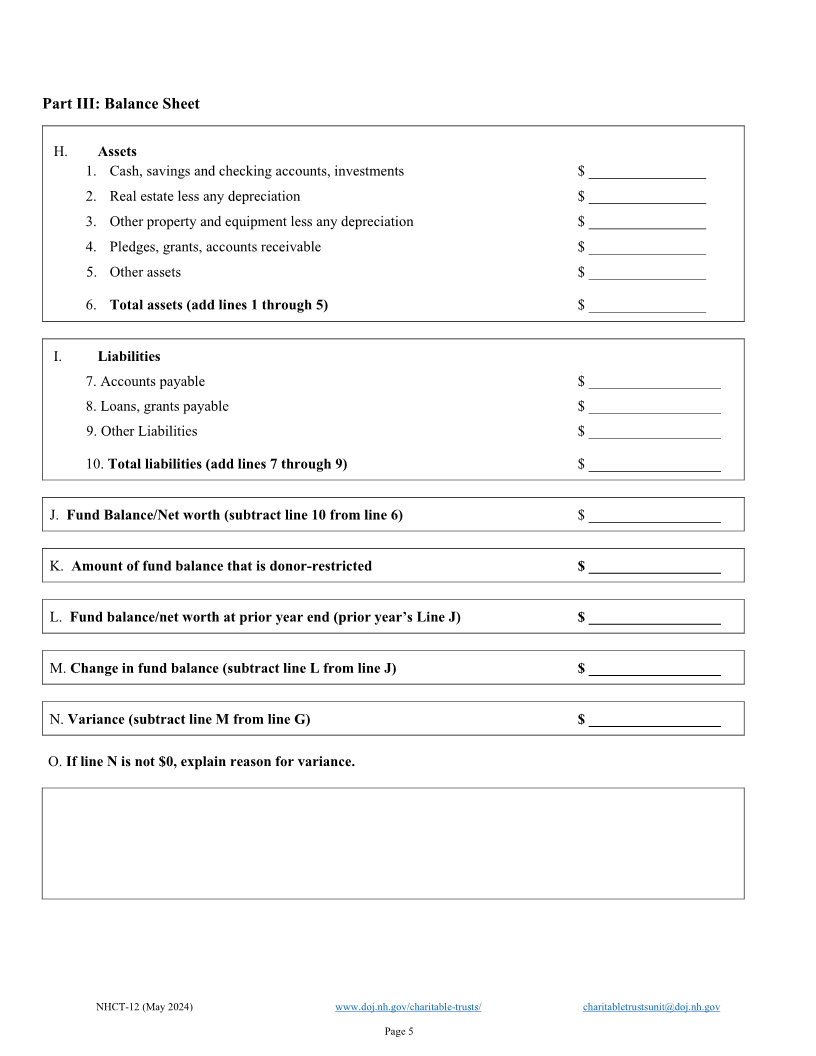
FORM NHCT-12
ANNUAL REPORT
*Instructions for the form are at the following web link:
https://www.doj.nh.gov/charitable-trusts/documents/nhct12-instructions.pdf
This form must be accompanied by a payment in the amount of $75.00, unless previously paid with Form
NHCT-14 for the reporting period. Checks must be made payable to “State of New Hampshire.”
Report is for fiscal year end date (MM/DD/YYYY): _______________________________
Is this a consolidated report for multiple years because the entity was granted a suspension of its annual
requirement?
□ Yes (if yes, state the beginning date of the consolidated report) __________________________________
□ No
CHARITABLE TRUST NFORMATIONI
NH Charitable Trusts Unit Registration No.
Entity Name □Check here if new name
City State Zip
Mailing Address □Check here if new address
Entity Website Address
CONTACT INFORMATION
Contact Name
Contact Address City State Zip
Contact Telephone Number
Contact Email Address
NHCT-12 (May 2024) www.doj.nh.gov/charitable-trusts/ charitabletrustsunit@doj.nh.gov
Page 1