Enlarge image
RPD-41358 State of New Mexico - Taxation and Revenue Department
Int. 09/05/2012
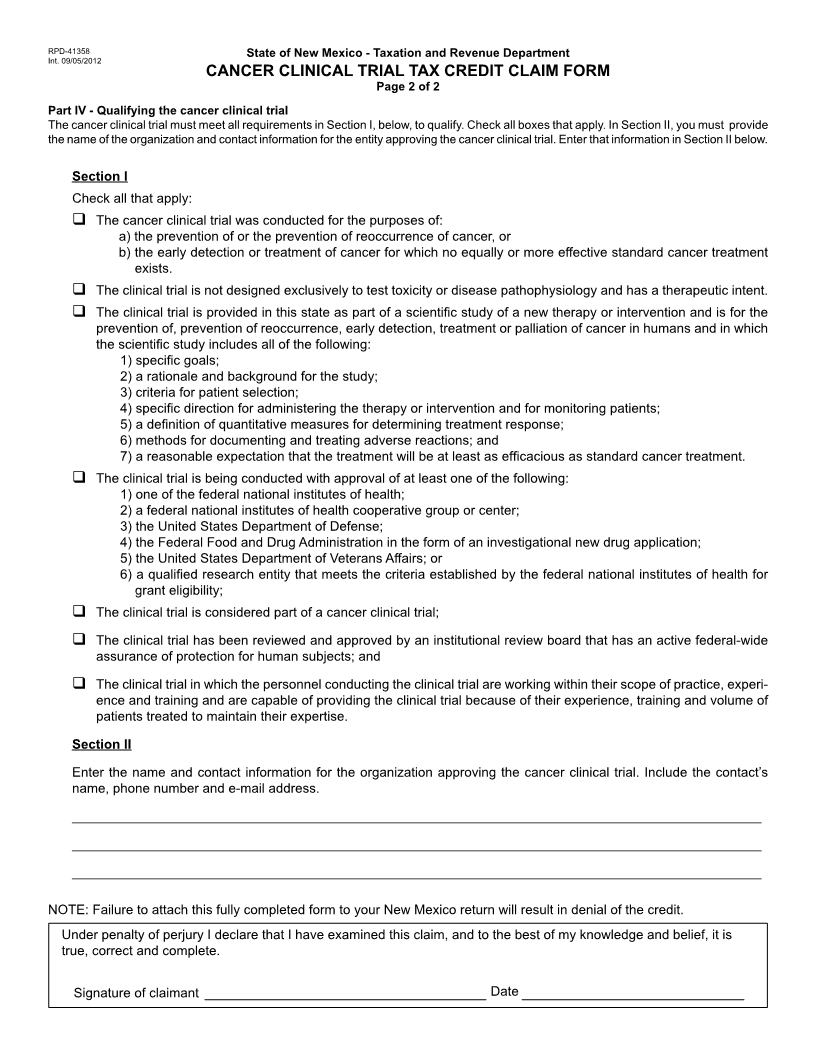
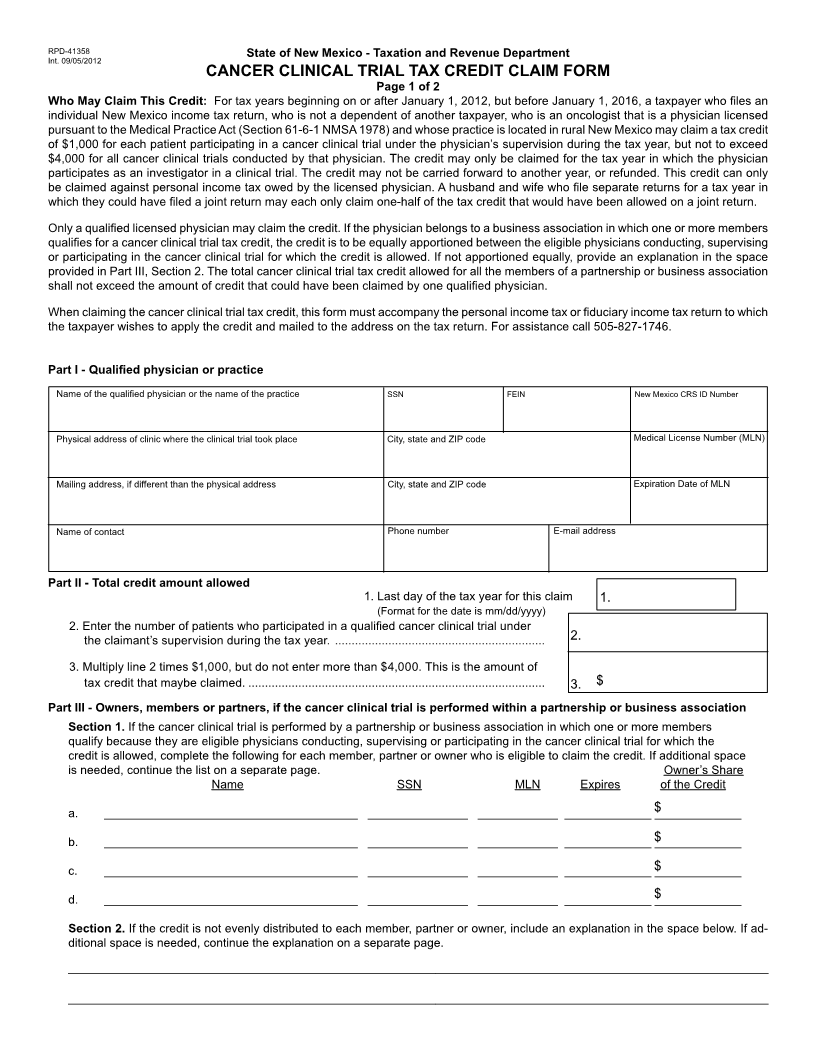
CANCER CLINICAL TRIAL TAX CREDIT CLAIM FORM
Page 1 of 2
Who May Claim This Credit: For tax years beginning on or after January 1, 2012, but before January 1, 2016, a taxpayer who les an
individual New Mexico income tax return, who is not a dependent of another taxpayer, who is an oncologist that is a physician licensed
pursuant to the Medical Practice Act (Section 61-6-1 NMSA 1978) and whose practice is located in rural New Mexico may claim a tax credit
of $1,000 for each patient participating in a cancer clinical trial under the physician’s supervision during the tax year, but not to exceed
$4,000 for all cancer clinical trials conducted by that physician. The credit may only be claimed for the tax year in which the physician
participates as an investigator in a clinical trial. The credit may not be carried forward to another year, or refunded. This credit can only
be claimed against personal income tax owed by the licensed physician. A husband and wife who le separate returns for a tax year in
which they could have led a joint return may each only claim one-half of the tax credit that would have been allowed on a joint return.
Only a qualied licensed physician may claim the credit. If the physician belongs to a business association in which one or more members
qualies for a cancer clinical trial tax credit, the credit is to be equally apportioned between the eligible physicians conducting, supervising
or participating in the cancer clinical trial for which the credit is allowed. If not apportioned equally, provide an explanation in the space
provided in Part III, Section 2. The total cancer clinical trial tax credit allowed for all the members of a partnership or business association
shall not exceed the amount of credit that could have been claimed by one qualied physician.
When claiming the cancer clinical trial tax credit, this form must accompany the personal income tax or duciary income tax return to which
the taxpayer wishes to apply the credit and mailed to the address on the tax return. For assistance call 505-827-1746.
Part I - Qualied physician or practice
Name of the qualied physician or the name of the practice SSN FEIN New Mexico CRS ID Number
Physical address of clinic where the clinical trial took place City, state and ZIP code Medical License Number (MLN)
Mailing address, if different than the physical address City, state and ZIP code Expiration Date of MLN
Phone number E-mail address
Name of contact
Part II - Total credit amount allowed
1. Last day of the tax year for this claim 1.
(Format for the date is mm/dd/yyyy)
2. Enter the number of patients who participated in a qualied cancer clinical trial under
the claimant’s supervision during the tax year. ............................................................... 2.
3. Multiply line 2 times $1,000, but do not enter more than $4,000. This is the amount of
tax credit that maybe claimed. ......................................................................................... 3. $
Part III - Owners, members or partners, if the cancer clinical trial is performed within a partnership or business association
Section 1. If the cancer clinical trial is performed by a partnership or business association in which one or more members
qualify because they are eligible physicians conducting, supervising or participating in the cancer clinical trial for which the
credit is allowed, complete the following for each member, partner or owner who is eligible to claim the credit. If additional space
is needed, continue the list on a separate page. Owner’s Share
Name SSN MLN Expires of the Credit
a. ______________________________________ _______________ ____________ _____________$_____________
b. ______________________________________ _______________ ____________ _____________$_____________
c. ______________________________________ _______________ ____________ _____________$_____________
d. ______________________________________ _______________ ____________ _____________$_____________
Section 2. If the credit is not evenly distributed to each member, partner or owner, include an explanation in the space below. If ad-
ditional space is needed, continue the explanation on a separate page.
________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________