Enlarge image
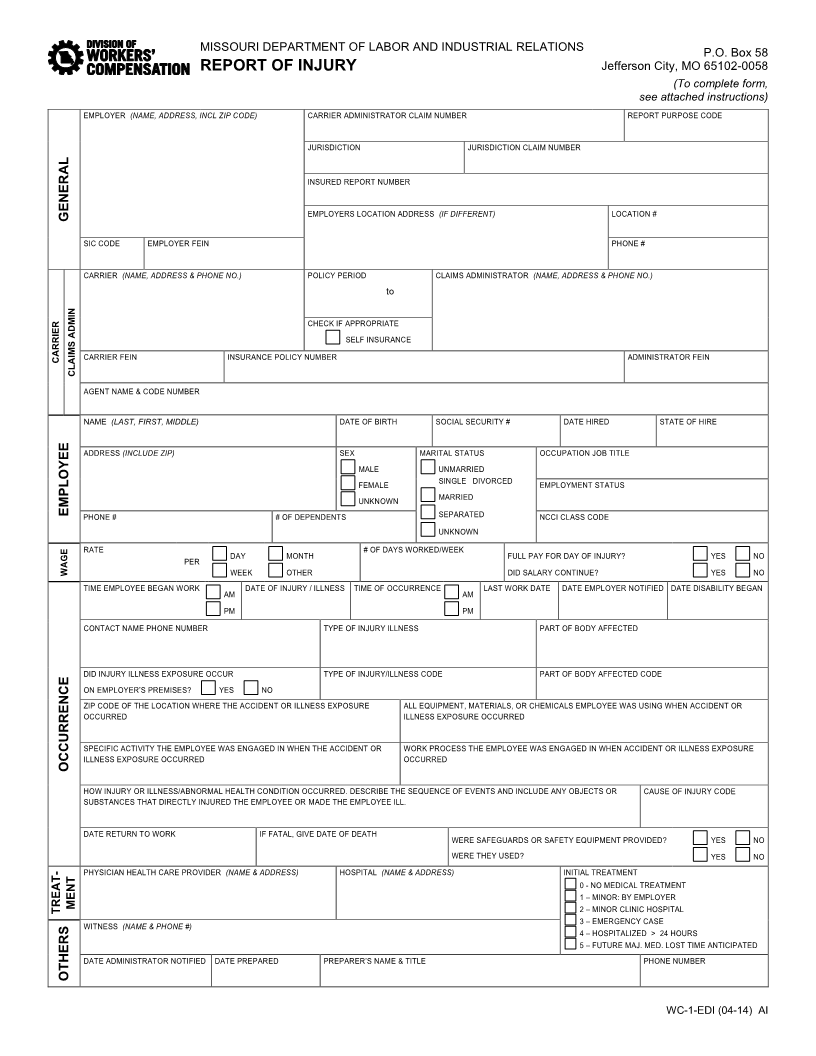
MISSOURI DEPARTMENT OF LABOR AND INDUSTRIAL RELATIONS P.O. Box 58
REPORT OF INJURY Jefferson City, MO 65102-0058
(To complete form,
see attached instructions)
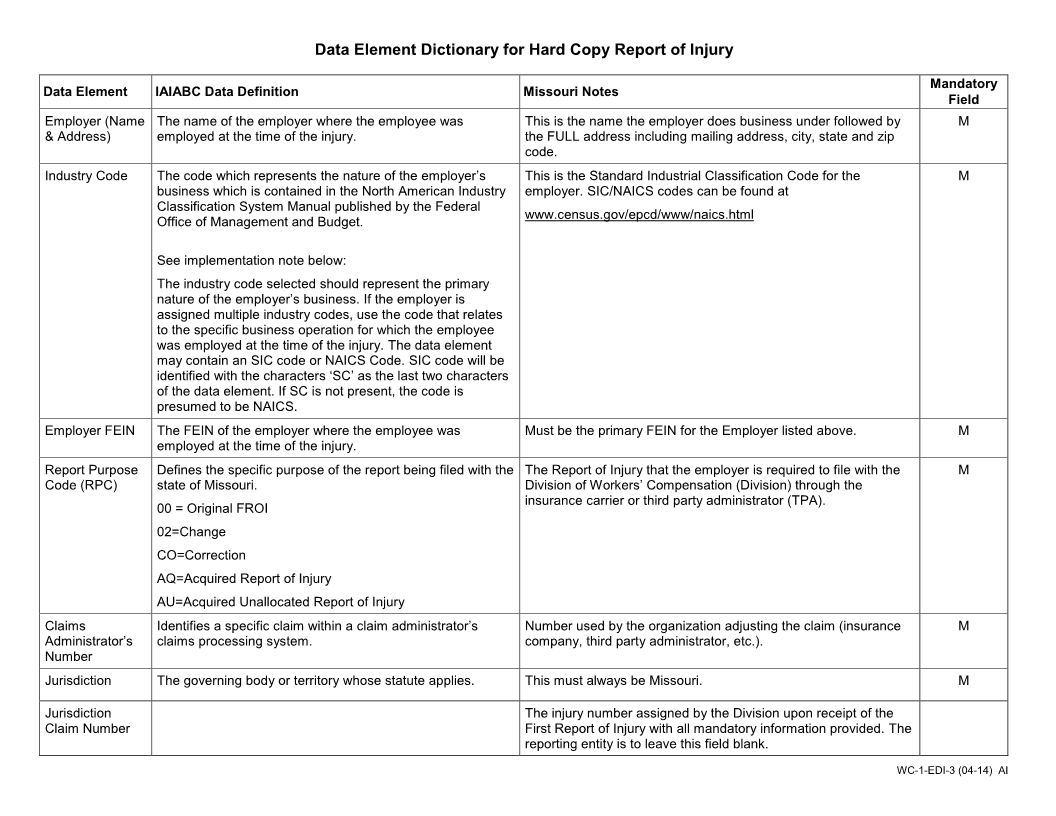
EMPLOYER (NAME, ADDRESS, INCL ZIP CODE) CARRIER ADMINISTRATOR CLAIM NUMBER REPORT PURPOSE CODE
JURISDICTION JURISDICTION CLAIM NUMBER
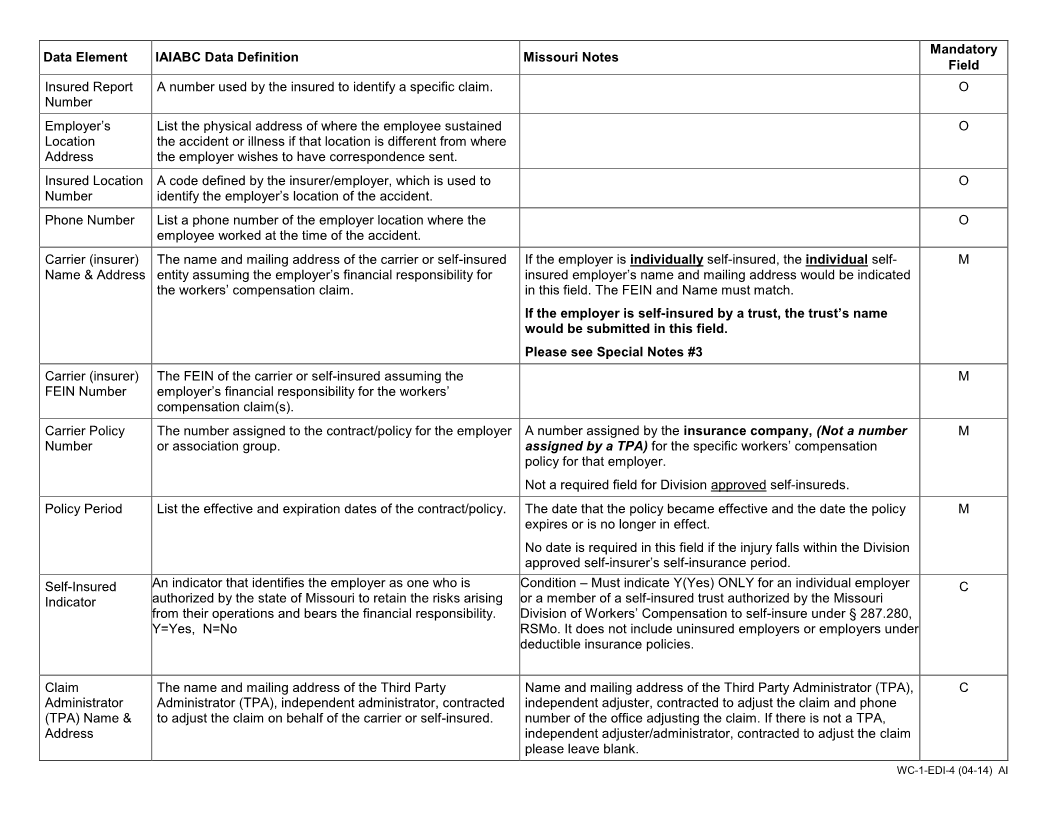
INSURED REPORT NUMBER
GENERAL EMPLOYERS LOCATION ADDRESS (IF DIFFERENT) LOCATION #
SIC CODE EMPLOYER FEIN PHONE #
CARRIER (NAME, ADDRESS & PHONE NO.) POLICY PERIOD CLAIMS ADMINISTRATOR (NAME, ADDRESS & PHONE NO.)
to
CHECK IF APPROPRIATE
SELF INSURANCE
CARRIER CARRIER FEIN INSURANCE POLICY NUMBER ADMINISTRATOR FEIN
CLAIMS ADMIN
AGENT NAME & CODE NUMBER
NAME (LAST, FIRST, MIDDLE) DATE OF BIRTH SOCIAL SECURITY # DATE HIRED STATE OF HIRE
ADDRESS (INCLUDE ZIP) SEX MARITAL STATUS OCCUPATION JOB TITLE
MALE UNMARRIED
FEMALE SINGLE DIVORCED EMPLOYMENT STATUS
UNKNOWN MARRIED
EMPLOYEE PHONE # # OF DEPENDENTS SEPARATED NCCI CLASS CODE
UNKNOWN
RATE
WAGE PER DAY MONTH # OF DAYS WORKED/WEEK FULL PAY FOR DAY OF INJURY? YES NO
WEEK OTHER DID SALARY CONTINUE? YES NO
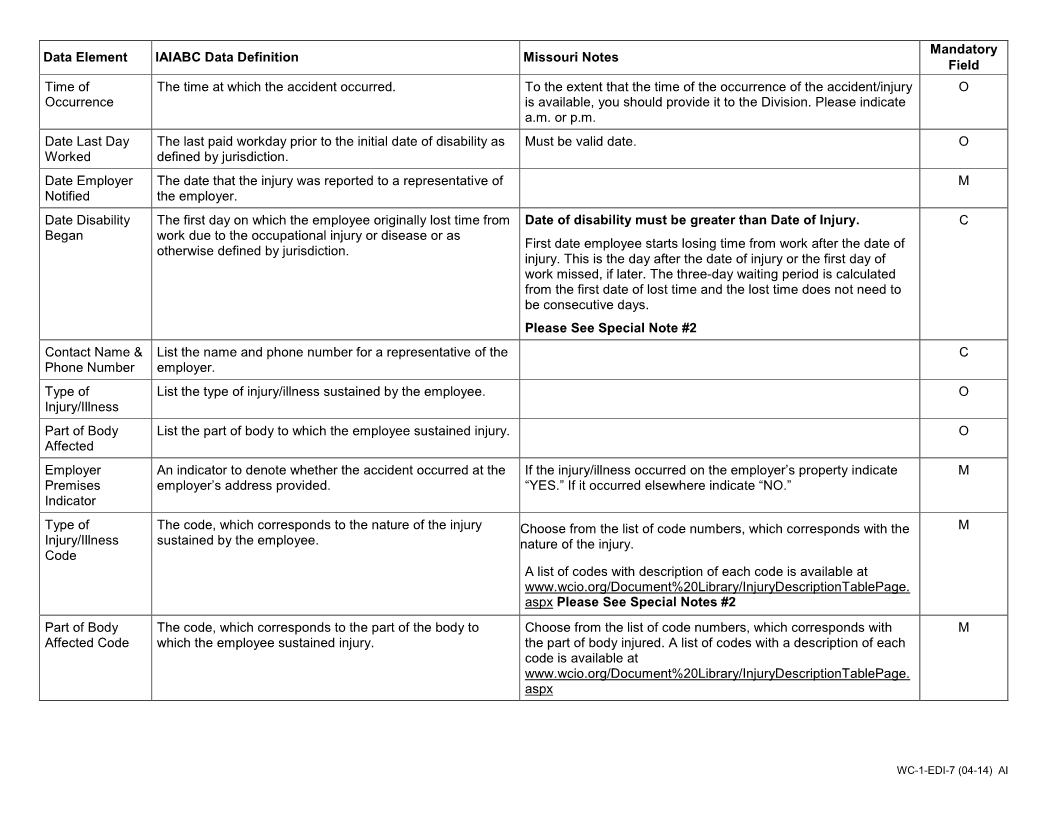
TIME EMPLOYEE BEGAN WORK AM DATE OF INJURY / ILLNESS TIME OF OCCURRENCE AM LAST WORK DATE DATE EMPLOYER NOTIFIED DATE DISABILITY BEGAN
PM PM
CONTACT NAME PHONE NUMBER TYPE OF INJURY ILLNESS PART OF BODY AFFECTED
DID INJURY ILLNESS EXPOSURE OCCUR TYPE OF INJURY/ILLNESS CODE PART OF BODY AFFECTED CODE
ON EMPLOYER’S PREMISES? YES NO
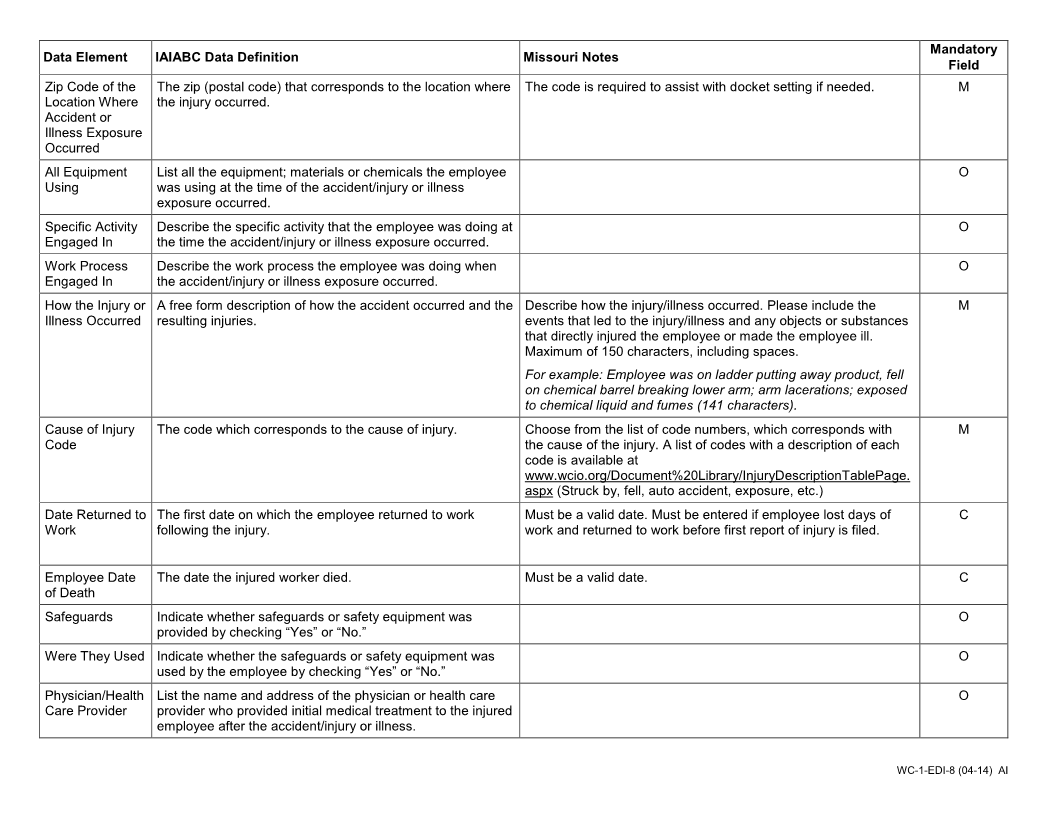
ZIP CODE OF THE LOCATION WHERE THE ACCIDENT OR ILLNESS EXPOSURE ALL EQUIPMENT, MATERIALS, OR CHEMICALS EMPLOYEE WAS USING WHEN ACCIDENT OR
OCCURRED ILLNESS EXPOSURE OCCURRED
SPECIFIC ACTIVITY THE EMPLOYEE WAS ENGAGED IN WHEN THE ACCIDENT OR WORK PROCESS THE EMPLOYEE WAS ENGAGED IN WHEN ACCIDENT OR ILLNESS EXPOSURE
ILLNESS EXPOSURE OCCURRED OCCURRED
OCCURRENCE
HOW INJURY OR ILLNESS/ABNORMAL HEALTH CONDITION OCCURRED. DESCRIBE THE SEQUENCE OF EVENTS AND INCLUDE ANY OBJECTS OR CAUSE OF INJURY CODE
SUBSTANCES THAT DIRECTLY INJURED THE EMPLOYEE OR MADE THE EMPLOYEE ILL.
DATE RETURN TO WORK IF FATAL, GIVE DATE OF DEATH WERE SAFEGUARDS OR SAFETY EQUIPMENT PROVIDED? YES NO
WERE THEY USED? YES NO
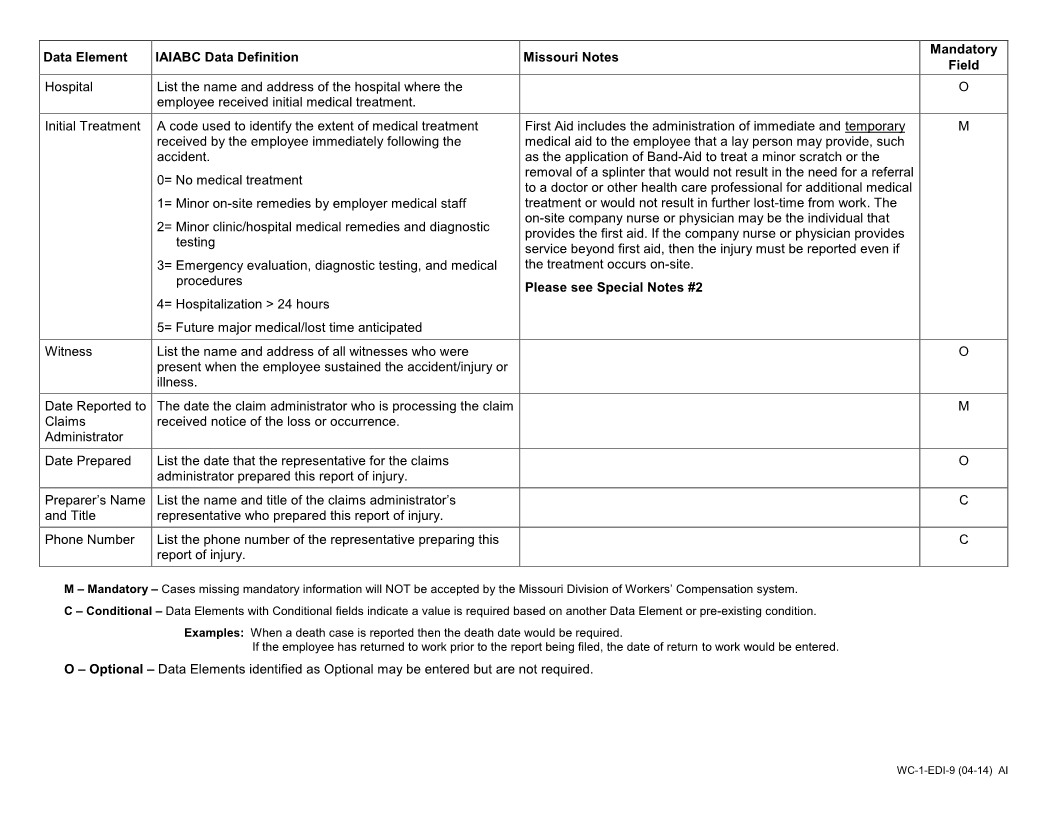
PHYSICIAN HEALTH CARE PROVIDER (NAME & ADDRESS) HOSPITAL (NAME & ADDRESS) INITIAL TREATMENT
0 - NO MEDICAL TREATMENT
1 – MINOR: BY EMPLOYER
TREAT- MENT 2 – MINOR CLINIC HOSPITAL
WITNESS (NAME & PHONE #) 3 – EMERGENCY CASE
4 – HOSPITALIZED > 24 HOURS
5 – FUTURE MAJ. MED. LOST TIME ANTICIPATED
DATE ADMINISTRATOR NOTIFIED DATE PREPARED PREPARER’S NAME & TITLE PHONE NUMBER
OTHERS
WC-1-EDI (04-14) AI